
Treasury Board of Canada Secretariat
www.tbs-sct.gc.ca
Common menu bar links
Breadcrumb Trail
ARCHIVED - Health Canada - Report
 This page has been archived.
This page has been archived.
Archived Content
Information identified as archived on the Web is for reference, research or recordkeeping purposes. It has not been altered or updated after the date of archiving. Web pages that are archived on the Web are not subject to the Government of Canada Web Standards. As per the Communications Policy of the Government of Canada, you can request alternate formats on the "Contact Us" page.
Minister's Message

As Canada's Minister of Health, I am pleased to present Health Canada's 2010-2011 Departmental Performance Report (DPR), which summarizes the department's accomplishments and its ongoing work to address key health priorities for this period. This report also summarizes Health Canada's progress in fulfilling its commitments to Canadians during the past year.
The department plays a critical role in leading efforts to promote and protect our health, to prevent illness and injury, to reduce disparities in health status, and to respond to emerging public health threats.
During the past year, we have made important progress in modernizing Canada's regulatory system for consumer products. On June 20, 2011, the Canada Consumer Product Safety Act came into force. This new law strengthens and modernizes our product-safety legislation to address emerging product-safety issues, and provides new ways to quickly and effectively protect Canadians from unsafe consumer products. At the same time, it responds to 21st-century technological and economic realities, such as globalization and the introduction of more complex consumer products.
Health Canada also addressed key priorities related to health products and food safety. Improvements to our regulatory processes are helping to ensure the ongoing availability of drugs and medical devices to Canadians. Enhanced labelling requirements for food allergens are helping consumers with food allergies to make informed choices. And Health Canada's new policy on Listeria, which provides for inspections and corrective measures concerning ready-to-eat foods, is helping to protect Canadian families from food-borne illnesses.
Our Government has made great strides to address health barriers facing First Nations and Inuit. We've strengthened our programming in critical areas such as diabetes and maternal and child health. Over the past two years, our investments through Canada's Economic Action Plan have brought 40 major building projects and 124 renovation projects from the drawing board to reality, resulting in better facilities for First Nations and Inuit, and for the people who provide key health services in Aboriginal communities. In addition, our Government has continued its work with provinces to better integrate First Nations health with provincial health systems.
Health Canada continues to work collaboratively with the provinces and territories to implement innovative approaches which respond to the health priorities and needs of Canadians, including access to health human resources. We will build on our progress in the years to come, so that all Canadians can enjoy the best health possible.
The Honourable Leona Aglukkaq, P.C., M.P.
Minister of Health
Section I: Departmental Overview
Raison d'�tre
Health Canada is responsible for helping Canadians maintain and improve their health. It is committed to improving the lives of all Canadians and to making this country's population among the healthiest in the world, as measured by longevity, lifestyle and effective use of the public health care system.
Responsibilities
Health Canada has many roles and responsibilities that help Canadians maintain and improve their health. First, as a regulator, Health Canada is responsible for the regulatory regime governing the safety of products including food, pharmaceuticals, medical devices, natural health products, consumer products, chemicals, radiation emitting devices, cosmetics and pesticides. It also regulates tobacco products and controlled substances, public health on aircraft, ships and other passenger conveyances, and helps manage the health risks posed by environmental factors such as air, water, radiation and contaminants.
The Department is also a service provider. The federal government has provided basic health services to First Nations since 1904. Today, Health Canada provides basic primary care services in approximately 200 remote First Nations communities, home and community care in 600 First Nations communities, support for health promotion programs in Inuit communities across four regions and a limited range of medically-necessary health-related goods and services not insured by private or other public health insurance plans to eligible First Nations and Inuit. The Department also funds or delivers community-based health programs and public health activities to First Nations and Inuit. These activities promote health, prevent chronic disease and address issues such as substance abuse and the spread of infectious diseases.
Health Canada is a catalyst for innovation, a funder, and an information provider in Canada's health system. It works closely with provincial and territorial governments to develop national approaches on health system issues and promotes the pan-Canadian adoption of best practices. It administers the Canada Health Act, which embodies national principles to ensure a universal and equitable publicly-funded health care system. It provides policy support for the federal government's Canada Health Transfer to provinces and territories, and provides funding through grants and contributions to various organizations to help meet Health Canada's objectives. Lastly, the Department draws on leading-edge science and policy research to generate and share knowledge and information to support decision-making by Canadians, development and implementation of regulations and standards, and health innovation.
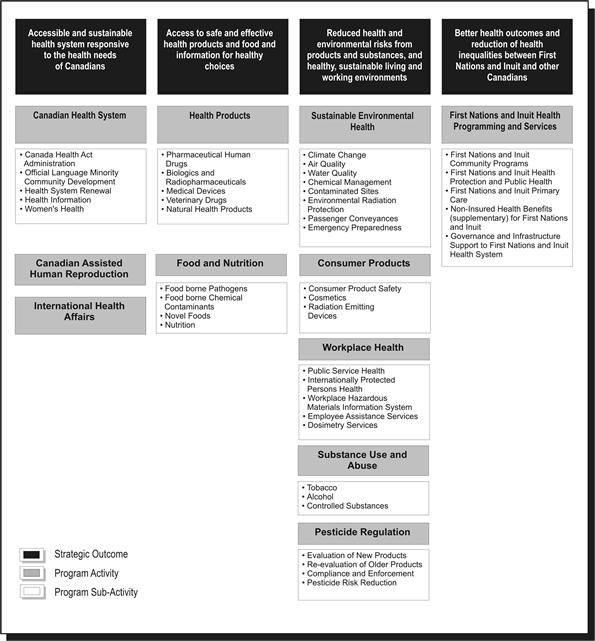
Strategic Outcome(s) and Program Activity Architecture (PAA)
In order to pursue its mandate most effectively and allocate resources appropriately, Health Canada has identified four strategic outcomes, each of which is supported by a framework of program activities and sub-activities.
Organizational Priorities
Priority Status Legend
Exceeded: More than 100 per cent of the expected level of performance for the priority identified in the corresponding RPP was achieved during the fiscal year.
Met All: 100 per cent of the expected level of performance for the priority identified in the corresponding RPP was achieved during the fiscal year
Mostly Met: 80 to 99 per cent of the expected level of performance for the priority identified in the corresponding RPP was achieved during the fiscal year.
Somewhat Met: 60 to 79 per cent of the expected level of performance for the priority identified in the corresponding RPP was achieved during the fiscal year.
Not Met: Less than 60 per cent of the expected level of performance for the priority identified in the corresponding RPP was achieved during the fiscal year.
| Organizational Priorities | Status |
|---|---|
| I. Modernized safety framework: | Type: Ongoing |
| Links to Strategic Outcomes: 2 and 3 | |
| The environment in which Health Canada carries out its legislated mandate to protect the health and safety of Canadians is changing rapidly. While the Department's track record on the safety of food and health, consumer and other products has been good, Health Canada has committed to regulatory modernization in order to deliver effective and efficient results in this changing environment. | |
| a) Continue to move forward with legislative proposals to enhance the protection of the health and safety of Canadians, including the Canada Consumer Product Safety Act, and proposed amendments to the Food and Drugs Act |
Met All Our department supported the Government in the process that led to the passage of the Canada Consumer Product Safety Act, which came into force in June 2011. While the Government did not proceed with amendments to Food and Drugs Act, we began a review of food and drug regulations for possible amendments in line with our modernization commitment. Parliament also approved updated user fees for drugs and medical devices that help to fund the modernization of our regulatory processes. |
| b) Increase consistency in the departmental regulatory approach across product areas |
Met All We worked towards a more consistent approach and streamlined regulatory functions across product lines. Our department began to integrate the compliance and enforcement functions that we deliver through our regional operations. We worked to develop a standard model and a more risk-based approach for our regulatory responsibilities. |
| c) Provide effective management of regulatory issues and emergency preparedness management |
Met All As a department with substantial regulatory responsibilities and the need to work effectively with the private sector, we identified and acted upon opportunities to improve our regulatory performance. We took steps to streamline processes, such as drafting regulatory amendments to reduce the backlog of proposed food additives. In response to demand for natural health products, we introduced the Unprocessed Product Licence Application Regulations, allowing for the legal sale of more than 6,000 products. Our department had a lead role in addressing the potential impacts on Canadians of radioactivity from Japanese nuclear power facilities after the March 2011 earthquake in Japan. We also initiated a process to allow the Canadian Red Cross to access medical supplies for humanitarian assistance in emergencies such as the cholera outbreak in Haiti. |
| d) In collaboration with partners, respond to recommendations and lessons learned from the listeriosis incident |
Met All We published new guidelines that represent the most comprehensive approach by a national food regulatory agency to prevent Listeria contamination of ready-to-eat foods during processing. The new risk-based approach guides Canadian Food Inspection Agency (CFIA) enforcement activities and is also a preventative tool to assist with early identification and mitigation of food contamination by Listeria. Our department also reviewed and communicated rapid methods to test for Listeria in the environment and in finished products for use by industry and CFIA. In addition, we reviewed and approved novel processes and applications to address possible contamination threats. |
| e) Continue implementation of the Chemicals Management Plan |
Met All Under the Chemicals Management Plan, we completed and published all scheduled risk assessments for 2010-2011 and published reports for other substances. We developed risk management strategies as necessary for chemicals in areas such as food products and pest control products. |
| II. Strengthen First Nations and Inuit health programming: | Type: Ongoing |
| Links to Strategic Outcomes: 4 | |
| While health outcomes for all Canadians are improving, First Nations and Inuit still experience serious health challenges. Health Canada continues to play an important role in supporting the delivery of, and access to, health programs and services for First Nations and Inuit. The Department is building on current departmental strategies, supported by additional funding in recent Budgets, in order to help further reduce the gap between health outcomes of First Nations and Inuit and those of other Canadians. | |
| a) Strengthen the First Nations health system |
Met All We collaborated with First Nations and government partners as well as stakeholders towards ensuring effective pandemic planning, prevention, mitigation and response strategies. The department also continued implementation of the $730 million over five years for Aboriginal health programs in Budget 2010, which are supporting and improving programs to address health priorities such as diabetes, youth suicide prevention and maternal child health. |
| b) Continue to explore potential to integrate and harmonize federal and provincial First Nations health programs and services through tripartite discussions |
Met All Negotiations in British Columbia involving Health Canada, the British Columbia government and First Nations partners resulted in a draft Framework Agreement for a new First Nations health governance arrangement in the province that moved to a ratification phase. Our Department also worked with the Saskatchewan government and First Nations partners to develop a 10-year Saskatchewan First Nations Health and Wellness Plan. |
| c) With funding from the Canada's Economic Action Plan, continue to strengthen the provision of primary care services to First Nations communities and non-insured health benefits coverage to First Nations and Inuit, and support new and renovated health infrastructure in First Nations communities |
Met All Canada's Economic Action Plan (CEAP) funding has accelerated the Department's long-term capital plan. Funding for more than 40 major capital projects and 135 minor renovation projects enabled us to build, replace, expand and improve First Nations health facilities such as health centres and nursing stations in all regions except the territories. These projects also created jobs in those communities. |
| d) Support health promotion and disease prevention in First Nations and Inuit communities |
Met All We launched, renewed or continued health promotion and disease prevention initiatives such as a campaign to increase awareness and understanding of infant immunization among First Nations and Inuit parents and caregivers. We also developed a new Infection Prevention and Control Strategy. We began to implement the funding announced in Budget 2010 that renewed important health promotion and disease prevention programs for First Nations and Inuit communities. This included the Aboriginal Diabetes Initiative, the National Aboriginal Youth Suicide Prevention Strategy, Maternal Child Health and Aboriginal Head Start On Reserve. |
| III. Health system innovation: | Type: Ongoing |
| Links to Strategic Outcomes: 1 | |
| The health care system in Canada is vital to addressing the health needs of Canadians wherever they live and whatever their financial circumstances. The health care system also has a significant economic impact, accounting for over 10% of Gross Domestic Product in 2008. Health Canada has a core role in promoting innovation to improve the effectiveness and efficiency of this system, with a particular emphasis on supporting efforts and collaboration by the provinces, territories and health system stakeholders. | |
| a) Continue to work with provincial and territorial governments as well as with other health care partners on health system sustainability, including measures to improve access to physicians, nurses and other health care providers for Canadians |
Met All We collaborated with provincial and territorial governments on innovations to improve access, effectiveness and efficiency in the Canadian health care system. These include initiatives to address the availability of health professionals, especially in underserved, rural and remote communities. Other projects are addressing issues in health care work environments to improve the retention and recruitment of nurses. Funding facilitated the integration of internationally educated health professionals into Canada's health care workforce. |
| b) Continue to work with Canada Health Infoway to accelerate the implementation of a pan-Canadian Electronic Health Record in collaboration with provincial and territorial governments. |
Met All We continued to support the development and implementation of eHealth technologies, such as electronic health records, electronic medical records and telehealth, through funding for Canada Health Infoway. |
| c) Collaborate with partners to address the medical imaging needs of Canadians. |
Met All In collaboration with the Canadian Agency for Drugs and Technologies in Health (CADTH), we supported an initiative to improve efficiency and effectiveness in the health system management of medical isotopes and alternate medical imaging technologies and approaches. |
| IV. Create a more collaborative, accountable and results-driven corporate culture | Type: Ongoing |
| Links to Strategic Outcomes: This management priority is part of the Internal Services program activity that contributes to all strategic outcomes | |
| The Department recognizes the value in getting our individual branches and program experts of many kinds to collaborate in pursuit of department-wide goals and with clearer accountability for generating results for Canadians. We also want Health Canada to offer workplaces that attract, retain and develop the diverse and skilled people who have the knowledge and expertise needed to deliver on our mandate. | |
| a) Update business models in areas of policy, science, regulation and regional program delivery, to create a more collaborative, responsible and results-driven corporate culture |
Met All We made progress on key commitments such as our Strategic Policy Renewal initiative and a departmental Science Plan to guide the development of policy frameworks and plans on health-related science policy issues. Our regional operations were reorganized to bring about an integrated and consistent approach to program delivery to Canadians and to achieve better results through efficiency, rapid response and consistency. |
| b) Continue to implement the Department's Talent Management Strategy and transformational initiatives to maximize investments in people at all levels and in all areas of expertise (e.g. the scientific and technology communities) |
Met All The new Health Canada Learning Strategy is designed to help enable our department to attract, develop, engage and retain the high performing workforce we need to deliver results for Canadians. We also developed a new Development Program Approach that aligns development with departmental business and organizational needs as well as an improved approach to official language training. |
| V. Enhance corporate processes for increased accountability: | Type: Ongoing |
| Links to Strategic Outcomes: This management priority is part of the Internal Services Program Activity which contributes to all strategic outcomes | |
| Health Canada is determined to improve how we establish and track accountability for resources and results. Improved measurement of performance and financial management helps ensure that we meet the expectations of Canadians. | |
| a) Increase the integration of planning, monitoring and reporting to improve information, with an emphasis on performance measurement, enabling decision-making affecting the Department's current and future operations |
Met All We made improvements across our corporate planning, accountability and reporting processes. These included a new Program Activity Architecture for 2011-2012 and improved performance measurement indicators. |
| b) Enhance the Financial Management Control Framework to ensure the effective allocation and monitoring of financial resources to achieve departmental objectives and priorities |
Met All We implemented action plans to ensure that our departmental accounts would align with our new Program Activity Architecture for the 2011-2012 fiscal year. |
| c) Increase the effectiveness of grants and contributions program management to provide for a more risk-based approach for decision-making to ensure a stronger focus on higher risk areas |
Met All We introduced a new Agreement/Recipient Risk Assessment Tool that supports risk management to improve management of grants and contributions programming. |
| VI. Increase transparency and innovative engagement with Canadians | Type: Ongoing |
| Links to Strategic Outcomes: This management priority is part of the Internal Services Program Activity which contributes to all strategic outcomes | |
| As a department with significant impacts on the lives of Canadians, it is important that Canadians can easily understand what we do as well as the information that we have and provide on their health and safety priorities. It is equally important that we are open and transparent in the planning and decision making on our important regulatory, policy and program responsibilities. | |
| a) Develop effective, up-to-date departmental tools and processes to engage Canadians |
Met All Our new tools and processes to engage Canadians included integrated strategic communications plans to support departmental initiatives such as the re-introduction of the Canada Consumer Product Safety Act and vehicles to communicate risk to Canadians. The department initiated, and in some cases completed, a variety of tools, policies and guidelines to improve our engagement of citizens and stakeholders in consultations. This included attention to how we work with our external advisory bodies. |
| b) Establish systematic, comprehensive departmental approaches to communicate and collaborate with stakeholders as well as engage citizens in the development, and review of departmental policies and programs |
Met All A department-wide initiative to improve the consistency and quality of Health Canada stakeholder and citizen engagement practices began in 2010-11. We also worked with external stakeholders to ensure consistent delivery of consumer-friendly information through tools such as the Consumer Safety Portal and created a team to focus on social media as a means to better reach Canadians. |
| c) Further implement means to ensure public access to timely, relevant health and safety information |
Met All Our department pursued marketing campaigns to support many of our policy and programs including the National Anti-Drug Strategy, the Food and Consumer Product Safety Action Plan as well as targeted education campaigns under the new Canadian Consumer Product Safety Act. |
Risk Analysis
Risk management is always significant for Health Canada. We work in an uncertain operational environment in which risks and incidents can emerge at any time that can require our department to shift management attention and resources rapidly. While we did not experience the kinds of major challenges in Canada that we had in previous years, we did address concerns about radiation threats after the March earthquake and tsunami in Japan seriously damaged the Fukushima Daiichi nuclear facility. To mitigate potential risks, we responded quickly and deployed additional nuclear radiation monitoring equipment to British Columbia. We also worked with the Canadian Food Inspection Agency (CFIA) to test imported foods for radiation and provided guidance to transportation industries on measures they could take to avoid potential radiation contamination. These helped reduce threats to Canadians.
Aside from that, our operations proceeded largely in line with our expectations set out in the Report on Plans and Priorities and we continued to address ongoing risks. One was the financial risk associated with the need to manage variable expenditures such as medical transportation in First Nation and Inuit communities under the Non-insured Health Benefits Program as well as unforeseeable events. In 2010-2011, we improved our Budget Management Framework and contingency planning to ensure that we forecast our resource needs effectively and spend those resources appropriately.
Human resources continued to be a Health Canada challenge. A risk to many of our critical services is our need for people in highly specialized fields who are also in high demand by other employers. For example, we have an ongoing need for health professionals in First Nations and Inuit communities and there is a shortage of scientists with the backgrounds needed to support our regulatory responsibilities. To help address these challenges, our department pursued the Aboriginal Health Human Resources Initiative and our Talent Management Strategy.
Health Canada manages a multitude of partnerships with other departments and with provincial, territorial and municipal governments, industry and non-governmental organizations. Our work with these partners helped us to share risks and learn from major health incidents such as the 2009 Listeria outbreak and international events such as the 2010 Winter Olympics and Paralympics. We have identified public awareness as a risk factor to manage, since Canadians look to us for timely, accurate and easy to find information in an era of globalization of health issues, new technologies and a 24-hour news cycle. We responded through actions such as an improved web presence and testing of social media tools.
Moving forward, Health Canada will draw upon experiences from 2010-2011 to identify risk drivers and manage uncertainties in 2011-2012 and beyond. By working across all programs to manage risk, the Department can concentrate efforts on gaps and priorities and relieve potential future pressures. These efforts also demonstrate the positive impacts of risk management and solidify its contribution to sound management practices.
Summary of Performance
2010-11 Financial Resources ($ millions)
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 3,448.5 | 3,859.6 | 3,752.6 |
2010-11 Human Resources (FTEs)
| Planned | Actual | Difference |
|---|---|---|
| 9,745 | 9,765 | 20 |
| Performance Indicators | Targets | 2010-11 Performance |
|---|---|---|
| Percentage of Canadians reporting timely access | Increased number of Canadians reporting timely access (baseline is 80% of Canadians reporting timely access taken from the Health Services Access Survey, published in 2006). | In 2009(**) 84.9% of Canadians, aged 12 and older, reported having a regular medical doctor, compared to 84.4% in 2008 and 84.9% in 2007. (*) The most recent figures from Statistics Canada show that most Canadians requiring routine or ongoing health services, health information or advice, and immediate care for a minor health problem do not report difficulties obtaining them. The percentage of Canadians self-reporting timely access to routine or ongoing health services was 82.8% in 2007, compared to 83.6% reported in 2003 and 2005.(*) The percentage of Canadians self-reporting timely access to immediate care for a minor health problem was 74.7% in 2007, compared to 79.3% in 2005 and 76.2 in 2003. The percentage of Canadians self-reporting timely access to health information or advice was 83.2% in 2007, compared to 85% in 2005 and 84.2% in 2003. |
| Percentage of Canadians satisfied with quality of primary, acute, chronic and continuing health care service | Increased number of Canadians satisfied with overall quality of health services (baseline is 85% of Canadians taken from Canadian Community Health Survey published in 2006). | In 2007, 85.2% of Canadians reported being "very satisfied" or "somewhat satisfied" with the way overall health care services were provided. Also, 89.8% of Canadians who received care from a physician reported being "very satisfied" or "somewhat satisfied" with the way physician care was provided. (*) |
| Increased sustainability of the health system through the development of new initiatives (long-term funding commitments, primary health care reform, use of science and technology) | Increased number of initiatives that improve sustainability in the health system. |
Initiatives relating to improved sustainability of the health care system included:
|
| Performance data is from either: (*) Healthy Canadians: A federal report on comparable health indicators, 2008 or (**) Statistics Canada. Cansim Table 105-0501 - Health indicator profile, annual estimates, by age group and sex, Canada, provinces, territories, health regions (2007 boundaries) and peer groups, occasional, CANSIM (database). | ||
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Canadian Health System | 369.4 | 297.3 | 297.3 | 385.9 | 377.5 | Healthy Canadians |
| Canadian Assisted Human Reproduction | 2.6 | 1.5 | 1.3 | 3.4 | 3.4 | |
| International Health Affairs | 19.3 | 21.2 | 21.3 | 21.8 | 18.7 | |
| Total | 391.3 | 320 | 319.9 | 411.1 | 399.6 | |
| Performance Indicators | Targets | 2010-11 Performance |
|---|---|---|
| Incidence/rate of illness/risk related to health products and food | Baseline information will be established in next two years | Many factors influence the incidence/rate of illness/risk related to food. |
| Increased rate of adherence to / compliance by industry with the Food and Drugs Act and its regulations, standards and guidelines |
Compliance:
|
|
| Increased public confidence in available information related to health products, food and nutrition | Year-over-year improvement of Canadians' confidence in the safety of the Canadian food supply | Spring 2010: 65% Fall 2010: 70% |
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Health Products | 191.2 | 144.7 | 144.7 | 176.1 | 170.6 | Healthy Canadians |
| Food and Nutrition | 41.5 | 66.7 | 69.7 | 70.6 | 58.4 | |
| Total | 232.7 | 211.4 | 214.4 | 246.7 | 229 | |
| Performance Indicators | Targets | 2010-11 Performance |
|---|---|---|
| Number of incidents of deaths, exposures, illness, injury and adverse reactions | Baseline information to be established in 2010-11 and 2011-12 for defined populations | No Baseline established for performance reporting |
| Proportion of regulatory actions addressed within service standards/targets | An average of 90% | No Baseline established for performance reporting |
| Percentage of inspected or verified registrants/firms/users compliant/non-compliant | Baseline information to be established in 2010-11 and 2011-12 for defined populations | No Baseline established for performance reporting |
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Sustainable Environmental Health | 130.5 | 130.4 | 152.2 | 141.1 | 134.9 | Healthy Canadians |
| Consumer Products | 27.3 | 31.7 | 33.9 | 33.6 | 27.9 | |
| Workplace Health | 35.7 | 20.1 | 20.2 | 31.7 | 31.7 | |
| Substance Use and Abuse | 104.6 | 133.6 | 133.6 | 140.8 | 124 | |
| Pesticide Regulation | 49.5 | 46.9 | 47 | 50.7 | 46.3 | |
| Total | 347.6 | 362.7 | 386.9 | 397.9 | 364.8 | |
| Performance Indicators* | Targets | 2010-11 Performance | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Life expectancy (at birth by gender, on and off reserve), comparison of First Nations and Inuit with other Canadians |
Reducing these inequalities. Interim targets for 2010/2011 (described in Section 2):
|
Life Expectancy (in years) for Canada (2000-2002), Registered Indians (2001) and Inuit-inhabited regions (1999-2003):
|
||||||||||||||||
| Birth weight (comparison of First Nations and Inuit with other Canadians) | Survey data from 2002-2003 indicate that 5.5% of First Nations on-reserve births were classified as low birth weight compared with 6.0% in Canada overall. The high birth weight rate for First Nations on-reserve was 21.0%, compared to the Canadian rate of 13.1%. The low birth weight rate among Inuit-inhabited areas (1990-2000) was 6.7% and the high birth weight rate was 13.1%. | |||||||||||||||||
| Infant mortality rates (comparison of First Nations with other Canadians) | First Nations infant mortality (IM) rates appear to have decreased, but remain approximately twice that of the non-First Nations population. IM rates within Inuit- regions are approximately four times the general population rate. | |||||||||||||||||
| Rates of conditions by type--e.g., diabetes, suicide | Diabetes for First Nations on-reserve was 3.8x higher compared to the rest of Canada in 2002-03. In 2005-06, diabetes for Inuit in Canada was 22% lower and the Inuit in Inuit Nunangat was 41% lower than the rest of Canada. The rate of First Nations youth suicide (10 to 19 years) was 4.3x greater than for Canada (2000). Suicide rate in Inuit regions (1999-2003) was 11.6x higher than for the rest of Canada. Most deaths by suicide in Inuit regions (1989-2003) were among males. |
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| First Nations and Inuit Health Programming and Services | 2,392.8 | 2,200.9 | 2,199.7 | 2,440.8 | 2,402.1 | Healthy Canadians |
| Total | 2,392.8 | 2,200.9 | 2,199.7 | 2,440.8 | 2,402.1 | |
* Note: Health Canada continues to work with federal (e.g. Statistics Canada, Aboriginal Affairs and Northern Development Canada) provincial and territorial partners as well as with First Nations and Inuit to improve the quality and accessibility of performance indicator data. Many indicators (e.g. life expectancy, mortality) only show changes over the very long-term.
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Internal Services* | 384.5 | 324.4 | 327.6 | 363.1 | 357.1 | Healthy Canadians |
| Total | 384.5 | 324.4 | 324.4 | 327.6 | 357.1 | |
* Note: Health Canada continues to work with federal (e.g. Statistics Canada, Aboriginal Affairs and Northern Development Canada) provincial and territorial partners as well as with First Nations and Inuit to improve the quality and accessibility of performance indicator data. Many indicators (e.g. life expectancy, mortality) only show changes over the very long-term.
Expenditure Profile
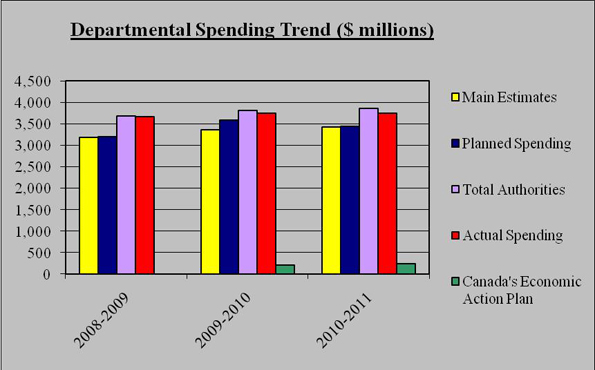
For the 2010-2011 fiscal year, Health Canada spent $3,752.6 million to meet expected program activity results and contribute to the achievement of departmental strategic outcomes. The figure below illustrates Health Canada's spending trend from 2008-09 to 2010-11.
Spending Trend
| 2010-2011 Departmental Spending Trend ($ millions) |
2008-2009 | 2009-2010 | 2010-11 |
|---|---|---|---|
| Main Estimates | 3,190.7 | 3,368.7 | 3,419.4 |
| Planned Spending | 3,195.3 | 3,587.0 | 3,448.5 |
| Total Authorities | 3,690.0 | 3,813.3 | 3,859.6 |
| Actual Spending | 3,668.1 | 3,748.9 | 3,752.6 |
| Canada's Economic Action Plan | 0.0 | 211.9 | 245.8 |
For Canada's Economic Action Plan in 2010-11 the table does not include the $500 million authorized in statutory funding for Canada Health Infoway and the corresponding $67.7 million in spending.
For the 2008-2009 to 2010-2011 periods, the total spending includes all Parliamentary appropriation sources: Main Estimates, Supplementary Estimates, Treasury Board collective bargaining, operating budget carry forward, and other special adjustments.
Departmental Spending Trend
The table below offers a comparison of the Main Estimates, planned spending, total authorities and actual spending for the most recently completed fiscal year, as well as the historical actual spending figures for the previous year.
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) |
|||
|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | ||
| Canadian Health System | 369.4 | 297.3 | 297.3 | 385.9 | 377.5 |
| Canadian Assisted Human Reproduction | 2.6 | 1.5 | 1.3 | 3.4 | 3.4 |
| International Health Affairs | 19.3 | 21.2 | 21.3 | 21.8 | 18.7 |
| Health Products | 191.2 | 144.7 | 144.7 | 176.1 | 170.6 |
| Food and Nutrition | 41.5 | 66.7 | 69.7 | 70.6 | 58.4 |
| Sustainable Environmental Health | 130.5 | 130.4 | 152.2 | 141.1 | 134.9 |
| Consumer Products | 27.3 | 31.7 | 33.9 | 33.6 | 27.9 |
| Workplace Health | 35.7 | 20.1 | 20.2 | 31.7 | 31.7 |
| Substance Use and Abuse | 104.6 | 133.6 | 133.6 | 140.8 | 124 |
| Pesticide Regulation | 49.5 | 46.9 | 47 | 50.7 | 46.3 |
| First Nations and Inuit Health Programming and Services | 2,392.8 | 2,200.9 | 2,199.7 | 2,440.8 | 2,402.1 |
| Internal Services | 384.5 | 324.4 | 327.6 | 363.1 | 357.1 |
| Total Department | 3,748.9 | 3,419.4 | 3.448.5 | 3,859.6 | 3,752.6 |
At the outset of the 2010-11 fiscal year, Health Canada's planned spending was $3,448.5 million. Through Main Estimates and Supplementary Estimates, our department was allocated total authorities of $3,859.6 million. Actual Health Canada spending was $3,752.6 million.
The $29.1 million increase from Main Estimates to Planned Spending is mainly due to fulfilling outstanding obligations under the Canadian Environmental Protection Act 1999.
The $411.1 million increase from planned spending to total authorities is mainly due to incremental funding for maintaining / improving current Aboriginal health promotion and disease prevention programs and the federal First nations and Inuit health systems; for providing mental health and emotional support services and research required to support the federal government's obligations under the Indian Residential Schools Agreement; and for grants to the governments of Nunavut, Northwest Territories and Yukon to support the Territorial Health System Sustainability Initiatives.
The $107 million difference between total authorities and actual spending is mainly the result of reprofile of funding to future years for programs like the National First Nations Public Health Surveillance projects and activities, the result of adjustments to plan related to timing of the passage of the Consumer Products Safety Act, frozen funding (i.e., subject to further release) for programs such as the National Anti-Drug Strategy, and some underspending in operating budgets.
Estimates by Vote
For information on our organizational votes and/or statutory expenditures, please see the 2010-11 Public Accounts of Canada (Volume II) publication.