ARCHIVED - Health Canada - Report
 This page has been archived.
This page has been archived.
Archived Content
Information identified as archived on the Web is for reference, research or recordkeeping purposes. It has not been altered or updated after the date of archiving. Web pages that are archived on the Web are not subject to the Government of Canada Web Standards. As per the Communications Policy of the Government of Canada, you can request alternate formats on the "Contact Us" page.
2010-11
Departmental Performance Report
Health Canada
The original version was signed by
The Honourable Leona Aglukkaq, P.C., M.P.
Minister of Health
Table of Contents
Section I: Organizational Overview
- Raison d'�tre
- Responsibilities
- Strategic Outcome(s) and Program Activity Architecture (PAA)
- Organizational Priorities
- Risk Analysis
- Summary of Performance
- Expenditure Profile
- Estimates by Vote
Section II: Analysis of Program Activities by Strategic Outcome
- Strategic Outcome #1
- Strategic Outcome #2
- Strategic Outcome #3
- Strategic Outcome #4
Section III: Supplementary Information
Minister's Message

As Canada's Minister of Health, I am pleased to present Health Canada's 2010-2011 Departmental Performance Report (DPR), which summarizes the department's accomplishments and its ongoing work to address key health priorities for this period. This report also summarizes Health Canada's progress in fulfilling its commitments to Canadians during the past year.
The department plays a critical role in leading efforts to promote and protect our health, to prevent illness and injury, to reduce disparities in health status, and to respond to emerging public health threats.
During the past year, we have made important progress in modernizing Canada's regulatory system for consumer products. On June 20, 2011, the Canada Consumer Product Safety Act came into force. This new law strengthens and modernizes our product-safety legislation to address emerging product-safety issues, and provides new ways to quickly and effectively protect Canadians from unsafe consumer products. At the same time, it responds to 21st-century technological and economic realities, such as globalization and the introduction of more complex consumer products.
Health Canada also addressed key priorities related to health products and food safety. Improvements to our regulatory processes are helping to ensure the ongoing availability of drugs and medical devices to Canadians. Enhanced labelling requirements for food allergens are helping consumers with food allergies to make informed choices. And Health Canada's new policy on Listeria, which provides for inspections and corrective measures concerning ready-to-eat foods, is helping to protect Canadian families from food-borne illnesses.
Our Government has made great strides to address health barriers facing First Nations and Inuit. We've strengthened our programming in critical areas such as diabetes and maternal and child health. Over the past two years, our investments through Canada's Economic Action Plan have brought 40 major building projects and 124 renovation projects from the drawing board to reality, resulting in better facilities for First Nations and Inuit, and for the people who provide key health services in Aboriginal communities. In addition, our Government has continued its work with provinces to better integrate First Nations health with provincial health systems.
Health Canada continues to work collaboratively with the provinces and territories to implement innovative approaches which respond to the health priorities and needs of Canadians, including access to health human resources. We will build on our progress in the years to come, so that all Canadians can enjoy the best health possible.
The Honourable Leona Aglukkaq, P.C., M.P.
Minister of Health
Section I: Departmental Overview
Raison d'�tre
Health Canada is responsible for helping Canadians maintain and improve their health. It is committed to improving the lives of all Canadians and to making this country's population among the healthiest in the world, as measured by longevity, lifestyle and effective use of the public health care system.
Responsibilities
Health Canada has many roles and responsibilities that help Canadians maintain and improve their health. First, as a regulator, Health Canada is responsible for the regulatory regime governing the safety of products including food, pharmaceuticals, medical devices, natural health products, consumer products, chemicals, radiation emitting devices, cosmetics and pesticides. It also regulates tobacco products and controlled substances, public health on aircraft, ships and other passenger conveyances, and helps manage the health risks posed by environmental factors such as air, water, radiation and contaminants.
The Department is also a service provider. The federal government has provided basic health services to First Nations since 1904. Today, Health Canada provides basic primary care services in approximately 200 remote First Nations communities, home and community care in 600 First Nations communities, support for health promotion programs in Inuit communities across four regions and a limited range of medically-necessary health-related goods and services not insured by private or other public health insurance plans to eligible First Nations and Inuit. The Department also funds or delivers community-based health programs and public health activities to First Nations and Inuit. These activities promote health, prevent chronic disease and address issues such as substance abuse and the spread of infectious diseases.
Health Canada is a catalyst for innovation, a funder, and an information provider in Canada's health system. It works closely with provincial and territorial governments to develop national approaches on health system issues and promotes the pan-Canadian adoption of best practices. It administers the Canada Health Act, which embodies national principles to ensure a universal and equitable publicly-funded health care system. It provides policy support for the federal government's Canada Health Transfer to provinces and territories, and provides funding through grants and contributions to various organizations to help meet Health Canada's objectives. Lastly, the Department draws on leading-edge science and policy research to generate and share knowledge and information to support decision-making by Canadians, development and implementation of regulations and standards, and health innovation.
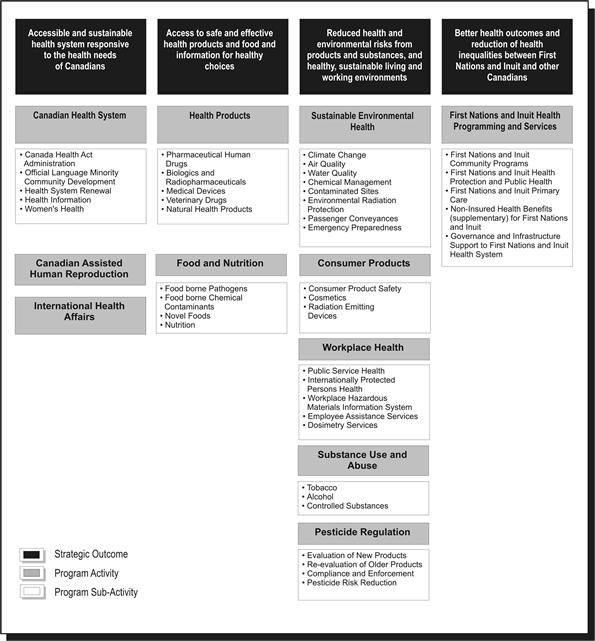
Strategic Outcome(s) and Program Activity Architecture (PAA)
In order to pursue its mandate most effectively and allocate resources appropriately, Health Canada has identified four strategic outcomes, each of which is supported by a framework of program activities and sub-activities.
Organizational Priorities
Priority Status Legend
Exceeded: More than 100 per cent of the expected level of performance for the priority identified in the corresponding RPP was achieved during the fiscal year.
Met All: 100 per cent of the expected level of performance for the priority identified in the corresponding RPP was achieved during the fiscal year
Mostly Met: 80 to 99 per cent of the expected level of performance for the priority identified in the corresponding RPP was achieved during the fiscal year.
Somewhat Met: 60 to 79 per cent of the expected level of performance for the priority identified in the corresponding RPP was achieved during the fiscal year.
Not Met: Less than 60 per cent of the expected level of performance for the priority identified in the corresponding RPP was achieved during the fiscal year.
| Organizational Priorities | Status |
|---|---|
| I. Modernized safety framework: | Type: Ongoing |
| Links to Strategic Outcomes: 2 and 3 | |
| The environment in which Health Canada carries out its legislated mandate to protect the health and safety of Canadians is changing rapidly. While the Department's track record on the safety of food and health, consumer and other products has been good, Health Canada has committed to regulatory modernization in order to deliver effective and efficient results in this changing environment. | |
| a) Continue to move forward with legislative proposals to enhance the protection of the health and safety of Canadians, including the Canada Consumer Product Safety Act, and proposed amendments to the Food and Drugs Act |
Met All Our department supported the Government in the process that led to the passage of the Canada Consumer Product Safety Act, which came into force in June 2011. While the Government did not proceed with amendments to Food and Drugs Act, we began a review of food and drug regulations for possible amendments in line with our modernization commitment. Parliament also approved updated user fees for drugs and medical devices that help to fund the modernization of our regulatory processes. |
| b) Increase consistency in the departmental regulatory approach across product areas |
Met All We worked towards a more consistent approach and streamlined regulatory functions across product lines. Our department began to integrate the compliance and enforcement functions that we deliver through our regional operations. We worked to develop a standard model and a more risk-based approach for our regulatory responsibilities. |
| c) Provide effective management of regulatory issues and emergency preparedness management |
Met All As a department with substantial regulatory responsibilities and the need to work effectively with the private sector, we identified and acted upon opportunities to improve our regulatory performance. We took steps to streamline processes, such as drafting regulatory amendments to reduce the backlog of proposed food additives. In response to demand for natural health products, we introduced the Unprocessed Product Licence Application Regulations, allowing for the legal sale of more than 6,000 products. Our department had a lead role in addressing the potential impacts on Canadians of radioactivity from Japanese nuclear power facilities after the March 2011 earthquake in Japan. We also initiated a process to allow the Canadian Red Cross to access medical supplies for humanitarian assistance in emergencies such as the cholera outbreak in Haiti. |
| d) In collaboration with partners, respond to recommendations and lessons learned from the listeriosis incident |
Met All We published new guidelines that represent the most comprehensive approach by a national food regulatory agency to prevent Listeria contamination of ready-to-eat foods during processing. The new risk-based approach guides Canadian Food Inspection Agency (CFIA) enforcement activities and is also a preventative tool to assist with early identification and mitigation of food contamination by Listeria. Our department also reviewed and communicated rapid methods to test for Listeria in the environment and in finished products for use by industry and CFIA. In addition, we reviewed and approved novel processes and applications to address possible contamination threats. |
| e) Continue implementation of the Chemicals Management Plan |
Met All Under the Chemicals Management Plan, we completed and published all scheduled risk assessments for 2010-2011 and published reports for other substances. We developed risk management strategies as necessary for chemicals in areas such as food products and pest control products. |
| II. Strengthen First Nations and Inuit health programming: | Type: Ongoing |
| Links to Strategic Outcomes: 4 | |
| While health outcomes for all Canadians are improving, First Nations and Inuit still experience serious health challenges. Health Canada continues to play an important role in supporting the delivery of, and access to, health programs and services for First Nations and Inuit. The Department is building on current departmental strategies, supported by additional funding in recent Budgets, in order to help further reduce the gap between health outcomes of First Nations and Inuit and those of other Canadians. | |
| a) Strengthen the First Nations health system |
Met All We collaborated with First Nations and government partners as well as stakeholders towards ensuring effective pandemic planning, prevention, mitigation and response strategies. The department also continued implementation of the $730 million over five years for Aboriginal health programs in Budget 2010, which are supporting and improving programs to address health priorities such as diabetes, youth suicide prevention and maternal child health. |
| b) Continue to explore potential to integrate and harmonize federal and provincial First Nations health programs and services through tripartite discussions |
Met All Negotiations in British Columbia involving Health Canada, the British Columbia government and First Nations partners resulted in a draft Framework Agreement for a new First Nations health governance arrangement in the province that moved to a ratification phase. Our Department also worked with the Saskatchewan government and First Nations partners to develop a 10-year Saskatchewan First Nations Health and Wellness Plan. |
| c) With funding from the Canada's Economic Action Plan, continue to strengthen the provision of primary care services to First Nations communities and non-insured health benefits coverage to First Nations and Inuit, and support new and renovated health infrastructure in First Nations communities |
Met All Canada's Economic Action Plan (CEAP) funding has accelerated the Department's long-term capital plan. Funding for more than 40 major capital projects and 135 minor renovation projects enabled us to build, replace, expand and improve First Nations health facilities such as health centres and nursing stations in all regions except the territories. These projects also created jobs in those communities. |
| d) Support health promotion and disease prevention in First Nations and Inuit communities |
Met All We launched, renewed or continued health promotion and disease prevention initiatives such as a campaign to increase awareness and understanding of infant immunization among First Nations and Inuit parents and caregivers. We also developed a new Infection Prevention and Control Strategy. We began to implement the funding announced in Budget 2010 that renewed important health promotion and disease prevention programs for First Nations and Inuit communities. This included the Aboriginal Diabetes Initiative, the National Aboriginal Youth Suicide Prevention Strategy, Maternal Child Health and Aboriginal Head Start On Reserve. |
| III. Health system innovation: | Type: Ongoing |
| Links to Strategic Outcomes: 1 | |
| The health care system in Canada is vital to addressing the health needs of Canadians wherever they live and whatever their financial circumstances. The health care system also has a significant economic impact, accounting for over 10% of Gross Domestic Product in 2008. Health Canada has a core role in promoting innovation to improve the effectiveness and efficiency of this system, with a particular emphasis on supporting efforts and collaboration by the provinces, territories and health system stakeholders. | |
| a) Continue to work with provincial and territorial governments as well as with other health care partners on health system sustainability, including measures to improve access to physicians, nurses and other health care providers for Canadians |
Met All We collaborated with provincial and territorial governments on innovations to improve access, effectiveness and efficiency in the Canadian health care system. These include initiatives to address the availability of health professionals, especially in underserved, rural and remote communities. Other projects are addressing issues in health care work environments to improve the retention and recruitment of nurses. Funding facilitated the integration of internationally educated health professionals into Canada's health care workforce. |
| b) Continue to work with Canada Health Infoway to accelerate the implementation of a pan-Canadian Electronic Health Record in collaboration with provincial and territorial governments. |
Met All We continued to support the development and implementation of eHealth technologies, such as electronic health records, electronic medical records and telehealth, through funding for Canada Health Infoway. |
| c) Collaborate with partners to address the medical imaging needs of Canadians. |
Met All In collaboration with the Canadian Agency for Drugs and Technologies in Health (CADTH), we supported an initiative to improve efficiency and effectiveness in the health system management of medical isotopes and alternate medical imaging technologies and approaches. |
| IV. Create a more collaborative, accountable and results-driven corporate culture | Type: Ongoing |
| Links to Strategic Outcomes: This management priority is part of the Internal Services program activity that contributes to all strategic outcomes | |
| The Department recognizes the value in getting our individual branches and program experts of many kinds to collaborate in pursuit of department-wide goals and with clearer accountability for generating results for Canadians. We also want Health Canada to offer workplaces that attract, retain and develop the diverse and skilled people who have the knowledge and expertise needed to deliver on our mandate. | |
| a) Update business models in areas of policy, science, regulation and regional program delivery, to create a more collaborative, responsible and results-driven corporate culture |
Met All We made progress on key commitments such as our Strategic Policy Renewal initiative and a departmental Science Plan to guide the development of policy frameworks and plans on health-related science policy issues. Our regional operations were reorganized to bring about an integrated and consistent approach to program delivery to Canadians and to achieve better results through efficiency, rapid response and consistency. |
| b) Continue to implement the Department's Talent Management Strategy and transformational initiatives to maximize investments in people at all levels and in all areas of expertise (e.g. the scientific and technology communities) |
Met All The new Health Canada Learning Strategy is designed to help enable our department to attract, develop, engage and retain the high performing workforce we need to deliver results for Canadians. We also developed a new Development Program Approach that aligns development with departmental business and organizational needs as well as an improved approach to official language training. |
| V. Enhance corporate processes for increased accountability: | Type: Ongoing |
| Links to Strategic Outcomes: This management priority is part of the Internal Services Program Activity which contributes to all strategic outcomes | |
| Health Canada is determined to improve how we establish and track accountability for resources and results. Improved measurement of performance and financial management helps ensure that we meet the expectations of Canadians. | |
| a) Increase the integration of planning, monitoring and reporting to improve information, with an emphasis on performance measurement, enabling decision-making affecting the Department's current and future operations |
Met All We made improvements across our corporate planning, accountability and reporting processes. These included a new Program Activity Architecture for 2011-2012 and improved performance measurement indicators. |
| b) Enhance the Financial Management Control Framework to ensure the effective allocation and monitoring of financial resources to achieve departmental objectives and priorities |
Met All We implemented action plans to ensure that our departmental accounts would align with our new Program Activity Architecture for the 2011-2012 fiscal year. |
| c) Increase the effectiveness of grants and contributions program management to provide for a more risk-based approach for decision-making to ensure a stronger focus on higher risk areas |
Met All We introduced a new Agreement/Recipient Risk Assessment Tool that supports risk management to improve management of grants and contributions programming. |
| VI. Increase transparency and innovative engagement with Canadians | Type: Ongoing |
| Links to Strategic Outcomes: This management priority is part of the Internal Services Program Activity which contributes to all strategic outcomes | |
| As a department with significant impacts on the lives of Canadians, it is important that Canadians can easily understand what we do as well as the information that we have and provide on their health and safety priorities. It is equally important that we are open and transparent in the planning and decision making on our important regulatory, policy and program responsibilities. | |
| a) Develop effective, up-to-date departmental tools and processes to engage Canadians |
Met All Our new tools and processes to engage Canadians included integrated strategic communications plans to support departmental initiatives such as the re-introduction of the Canada Consumer Product Safety Act and vehicles to communicate risk to Canadians. The department initiated, and in some cases completed, a variety of tools, policies and guidelines to improve our engagement of citizens and stakeholders in consultations. This included attention to how we work with our external advisory bodies. |
| b) Establish systematic, comprehensive departmental approaches to communicate and collaborate with stakeholders as well as engage citizens in the development, and review of departmental policies and programs |
Met All A department-wide initiative to improve the consistency and quality of Health Canada stakeholder and citizen engagement practices began in 2010-11. We also worked with external stakeholders to ensure consistent delivery of consumer-friendly information through tools such as the Consumer Safety Portal and created a team to focus on social media as a means to better reach Canadians. |
| c) Further implement means to ensure public access to timely, relevant health and safety information |
Met All Our department pursued marketing campaigns to support many of our policy and programs including the National Anti-Drug Strategy, the Food and Consumer Product Safety Action Plan as well as targeted education campaigns under the new Canadian Consumer Product Safety Act. |
Risk Analysis
Risk management is always significant for Health Canada. We work in an uncertain operational environment in which risks and incidents can emerge at any time that can require our department to shift management attention and resources rapidly. While we did not experience the kinds of major challenges in Canada that we had in previous years, we did address concerns about radiation threats after the March earthquake and tsunami in Japan seriously damaged the Fukushima Daiichi nuclear facility. To mitigate potential risks, we responded quickly and deployed additional nuclear radiation monitoring equipment to British Columbia. We also worked with the Canadian Food Inspection Agency (CFIA) to test imported foods for radiation and provided guidance to transportation industries on measures they could take to avoid potential radiation contamination. These helped reduce threats to Canadians.
Aside from that, our operations proceeded largely in line with our expectations set out in the Report on Plans and Priorities and we continued to address ongoing risks. One was the financial risk associated with the need to manage variable expenditures such as medical transportation in First Nation and Inuit communities under the Non-insured Health Benefits Program as well as unforeseeable events. In 2010-2011, we improved our Budget Management Framework and contingency planning to ensure that we forecast our resource needs effectively and spend those resources appropriately.
Human resources continued to be a Health Canada challenge. A risk to many of our critical services is our need for people in highly specialized fields who are also in high demand by other employers. For example, we have an ongoing need for health professionals in First Nations and Inuit communities and there is a shortage of scientists with the backgrounds needed to support our regulatory responsibilities. To help address these challenges, our department pursued the Aboriginal Health Human Resources Initiative and our Talent Management Strategy.
Health Canada manages a multitude of partnerships with other departments and with provincial, territorial and municipal governments, industry and non-governmental organizations. Our work with these partners helped us to share risks and learn from major health incidents such as the 2009 Listeria outbreak and international events such as the 2010 Winter Olympics and Paralympics. We have identified public awareness as a risk factor to manage, since Canadians look to us for timely, accurate and easy to find information in an era of globalization of health issues, new technologies and a 24-hour news cycle. We responded through actions such as an improved web presence and testing of social media tools.
Moving forward, Health Canada will draw upon experiences from 2010-2011 to identify risk drivers and manage uncertainties in 2011-2012 and beyond. By working across all programs to manage risk, the Department can concentrate efforts on gaps and priorities and relieve potential future pressures. These efforts also demonstrate the positive impacts of risk management and solidify its contribution to sound management practices.
Summary of Performance
2010-11 Financial Resources ($ millions)
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 3,448.5 | 3,859.6 | 3,752.6 |
2010-11 Human Resources (FTEs)
| Planned | Actual | Difference |
|---|---|---|
| 9,745 | 9,765 | 20 |
| Performance Indicators | Targets | 2010-11 Performance |
|---|---|---|
| Percentage of Canadians reporting timely access | Increased number of Canadians reporting timely access (baseline is 80% of Canadians reporting timely access taken from the Health Services Access Survey, published in 2006). | In 2009(**) 84.9% of Canadians, aged 12 and older, reported having a regular medical doctor, compared to 84.4% in 2008 and 84.9% in 2007. (*) The most recent figures from Statistics Canada show that most Canadians requiring routine or ongoing health services, health information or advice, and immediate care for a minor health problem do not report difficulties obtaining them. The percentage of Canadians self-reporting timely access to routine or ongoing health services was 82.8% in 2007, compared to 83.6% reported in 2003 and 2005.(*) The percentage of Canadians self-reporting timely access to immediate care for a minor health problem was 74.7% in 2007, compared to 79.3% in 2005 and 76.2 in 2003. The percentage of Canadians self-reporting timely access to health information or advice was 83.2% in 2007, compared to 85% in 2005 and 84.2% in 2003. |
| Percentage of Canadians satisfied with quality of primary, acute, chronic and continuing health care service | Increased number of Canadians satisfied with overall quality of health services (baseline is 85% of Canadians taken from Canadian Community Health Survey published in 2006). | In 2007, 85.2% of Canadians reported being "very satisfied" or "somewhat satisfied" with the way overall health care services were provided. Also, 89.8% of Canadians who received care from a physician reported being "very satisfied" or "somewhat satisfied" with the way physician care was provided. (*) |
| Increased sustainability of the health system through the development of new initiatives (long-term funding commitments, primary health care reform, use of science and technology) | Increased number of initiatives that improve sustainability in the health system. |
Initiatives relating to improved sustainability of the health care system included:
|
| Performance data is from either: (*) Healthy Canadians: A federal report on comparable health indicators, 2008 or (**) Statistics Canada. Cansim Table 105-0501 - Health indicator profile, annual estimates, by age group and sex, Canada, provinces, territories, health regions (2007 boundaries) and peer groups, occasional, CANSIM (database). | ||
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Canadian Health System | 369.4 | 297.3 | 297.3 | 385.9 | 377.5 | Healthy Canadians |
| Canadian Assisted Human Reproduction | 2.6 | 1.5 | 1.3 | 3.4 | 3.4 | |
| International Health Affairs | 19.3 | 21.2 | 21.3 | 21.8 | 18.7 | |
| Total | 391.3 | 320 | 319.9 | 411.1 | 399.6 | |
| Performance Indicators | Targets | 2010-11 Performance |
|---|---|---|
| Incidence/rate of illness/risk related to health products and food | Baseline information will be established in next two years | Many factors influence the incidence/rate of illness/risk related to food. |
| Increased rate of adherence to / compliance by industry with the Food and Drugs Act and its regulations, standards and guidelines |
Compliance:
|
|
| Increased public confidence in available information related to health products, food and nutrition | Year-over-year improvement of Canadians' confidence in the safety of the Canadian food supply | Spring 2010: 65% Fall 2010: 70% |
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Health Products | 191.2 | 144.7 | 144.7 | 176.1 | 170.6 | Healthy Canadians |
| Food and Nutrition | 41.5 | 66.7 | 69.7 | 70.6 | 58.4 | |
| Total | 232.7 | 211.4 | 214.4 | 246.7 | 229 | |
| Performance Indicators | Targets | 2010-11 Performance |
|---|---|---|
| Number of incidents of deaths, exposures, illness, injury and adverse reactions | Baseline information to be established in 2010-11 and 2011-12 for defined populations | No Baseline established for performance reporting |
| Proportion of regulatory actions addressed within service standards/targets | An average of 90% | No Baseline established for performance reporting |
| Percentage of inspected or verified registrants/firms/users compliant/non-compliant | Baseline information to be established in 2010-11 and 2011-12 for defined populations | No Baseline established for performance reporting |
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Sustainable Environmental Health | 130.5 | 130.4 | 152.2 | 141.1 | 134.9 | Healthy Canadians |
| Consumer Products | 27.3 | 31.7 | 33.9 | 33.6 | 27.9 | |
| Workplace Health | 35.7 | 20.1 | 20.2 | 31.7 | 31.7 | |
| Substance Use and Abuse | 104.6 | 133.6 | 133.6 | 140.8 | 124 | |
| Pesticide Regulation | 49.5 | 46.9 | 47 | 50.7 | 46.3 | |
| Total | 347.6 | 362.7 | 386.9 | 397.9 | 364.8 | |
| Performance Indicators* | Targets | 2010-11 Performance | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Life expectancy (at birth by gender, on and off reserve), comparison of First Nations and Inuit with other Canadians |
Reducing these inequalities. Interim targets for 2010/2011 (described in Section 2):
|
Life Expectancy (in years) for Canada (2000-2002), Registered Indians (2001) and Inuit-inhabited regions (1999-2003):
|
||||||||||||||||
| Birth weight (comparison of First Nations and Inuit with other Canadians) | Survey data from 2002-2003 indicate that 5.5% of First Nations on-reserve births were classified as low birth weight compared with 6.0% in Canada overall. The high birth weight rate for First Nations on-reserve was 21.0%, compared to the Canadian rate of 13.1%. The low birth weight rate among Inuit-inhabited areas (1990-2000) was 6.7% and the high birth weight rate was 13.1%. | |||||||||||||||||
| Infant mortality rates (comparison of First Nations with other Canadians) | First Nations infant mortality (IM) rates appear to have decreased, but remain approximately twice that of the non-First Nations population. IM rates within Inuit- regions are approximately four times the general population rate. | |||||||||||||||||
| Rates of conditions by type--e.g., diabetes, suicide | Diabetes for First Nations on-reserve was 3.8x higher compared to the rest of Canada in 2002-03. In 2005-06, diabetes for Inuit in Canada was 22% lower and the Inuit in Inuit Nunangat was 41% lower than the rest of Canada. The rate of First Nations youth suicide (10 to 19 years) was 4.3x greater than for Canada (2000). Suicide rate in Inuit regions (1999-2003) was 11.6x higher than for the rest of Canada. Most deaths by suicide in Inuit regions (1989-2003) were among males. |
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| First Nations and Inuit Health Programming and Services | 2,392.8 | 2,200.9 | 2,199.7 | 2,440.8 | 2,402.1 | Healthy Canadians |
| Total | 2,392.8 | 2,200.9 | 2,199.7 | 2,440.8 | 2,402.1 | |
* Note: Health Canada continues to work with federal (e.g. Statistics Canada, Aboriginal Affairs and Northern Development Canada) provincial and territorial partners as well as with First Nations and Inuit to improve the quality and accessibility of performance indicator data. Many indicators (e.g. life expectancy, mortality) only show changes over the very long-term.
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Internal Services* | 384.5 | 324.4 | 327.6 | 363.1 | 357.1 | Healthy Canadians |
| Total | 384.5 | 324.4 | 324.4 | 327.6 | 357.1 | |
* Note: Health Canada continues to work with federal (e.g. Statistics Canada, Aboriginal Affairs and Northern Development Canada) provincial and territorial partners as well as with First Nations and Inuit to improve the quality and accessibility of performance indicator data. Many indicators (e.g. life expectancy, mortality) only show changes over the very long-term.
Expenditure Profile
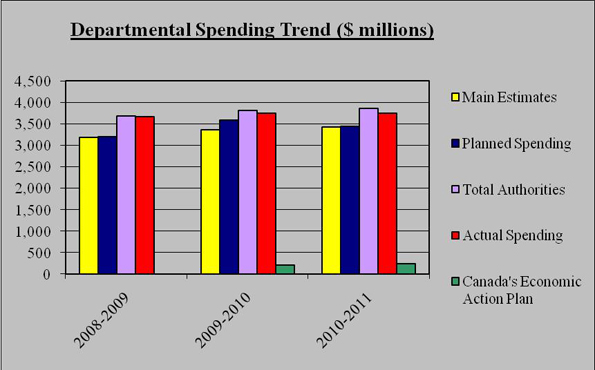
For the 2010-2011 fiscal year, Health Canada spent $3,752.6 million to meet expected program activity results and contribute to the achievement of departmental strategic outcomes. The figure below illustrates Health Canada's spending trend from 2008-09 to 2010-11.
Spending Trend
| 2010-2011 Departmental Spending Trend ($ millions) |
2008-2009 | 2009-2010 | 2010-11 |
|---|---|---|---|
| Main Estimates | 3,190.7 | 3,368.7 | 3,419.4 |
| Planned Spending | 3,195.3 | 3,587.0 | 3,448.5 |
| Total Authorities | 3,690.0 | 3,813.3 | 3,859.6 |
| Actual Spending | 3,668.1 | 3,748.9 | 3,752.6 |
| Canada's Economic Action Plan | 0.0 | 211.9 | 245.8 |
For Canada's Economic Action Plan in 2010-11 the table does not include the $500 million authorized in statutory funding for Canada Health Infoway and the corresponding $67.7 million in spending.
For the 2008-2009 to 2010-2011 periods, the total spending includes all Parliamentary appropriation sources: Main Estimates, Supplementary Estimates, Treasury Board collective bargaining, operating budget carry forward, and other special adjustments.
Departmental Spending Trend
The table below offers a comparison of the Main Estimates, planned spending, total authorities and actual spending for the most recently completed fiscal year, as well as the historical actual spending figures for the previous year.
| Program Activity | 2009-10 Actual Spending ($ millions) |
2010-11 ($ millions) |
|||
|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | ||
| Canadian Health System | 369.4 | 297.3 | 297.3 | 385.9 | 377.5 |
| Canadian Assisted Human Reproduction | 2.6 | 1.5 | 1.3 | 3.4 | 3.4 |
| International Health Affairs | 19.3 | 21.2 | 21.3 | 21.8 | 18.7 |
| Health Products | 191.2 | 144.7 | 144.7 | 176.1 | 170.6 |
| Food and Nutrition | 41.5 | 66.7 | 69.7 | 70.6 | 58.4 |
| Sustainable Environmental Health | 130.5 | 130.4 | 152.2 | 141.1 | 134.9 |
| Consumer Products | 27.3 | 31.7 | 33.9 | 33.6 | 27.9 |
| Workplace Health | 35.7 | 20.1 | 20.2 | 31.7 | 31.7 |
| Substance Use and Abuse | 104.6 | 133.6 | 133.6 | 140.8 | 124 |
| Pesticide Regulation | 49.5 | 46.9 | 47 | 50.7 | 46.3 |
| First Nations and Inuit Health Programming and Services | 2,392.8 | 2,200.9 | 2,199.7 | 2,440.8 | 2,402.1 |
| Internal Services | 384.5 | 324.4 | 327.6 | 363.1 | 357.1 |
| Total Department | 3,748.9 | 3,419.4 | 3.448.5 | 3,859.6 | 3,752.6 |
At the outset of the 2010-11 fiscal year, Health Canada's planned spending was $3,448.5 million. Through Main Estimates and Supplementary Estimates, our department was allocated total authorities of $3,859.6 million. Actual Health Canada spending was $3,752.6 million.
The $29.1 million increase from Main Estimates to Planned Spending is mainly due to fulfilling outstanding obligations under the Canadian Environmental Protection Act 1999.
The $411.1 million increase from planned spending to total authorities is mainly due to incremental funding for maintaining / improving current Aboriginal health promotion and disease prevention programs and the federal First nations and Inuit health systems; for providing mental health and emotional support services and research required to support the federal government's obligations under the Indian Residential Schools Agreement; and for grants to the governments of Nunavut, Northwest Territories and Yukon to support the Territorial Health System Sustainability Initiatives.
The $107 million difference between total authorities and actual spending is mainly the result of reprofile of funding to future years for programs like the National First Nations Public Health Surveillance projects and activities, the result of adjustments to plan related to timing of the passage of the Consumer Products Safety Act, frozen funding (i.e., subject to further release) for programs such as the National Anti-Drug Strategy, and some underspending in operating budgets.
Estimates by Vote
For information on our organizational votes and/or statutory expenditures, please see the 2010-11 Public Accounts of Canada (Volume II) publication.
Section II: Analysis of Program Activities by Strategic Outcome
Strategic Outcome #1
Maintaining the accessibility and sustainability of Canada's health system is a shared responsibility requiring Health Canada to work closely with provincial and territorial governments, as well as health organizations and other stakeholder groups. Our Department continually examines new and innovative approaches and responses to the health priorities and needs of Canadians.
Serving as a partner, an enabler, an innovator, a knowledge broker and a proponent of transparency and accountability, Health Canada plays a role in supporting the sustainability of Canada's health system. To Canadians, sustainability means the availability, maintenance and advancement of key attributes of Canada's publicly funded health system such as accessibility, efficiency and effectiveness. In the face of perpetually shifting and growing health system demands, the Department develops policies in support of a sustainable health system for Canadians.
Program Activity 1: Canadian Health System

Program Activity Descriptions
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 297.3 | 385.9 | 377.5 |
| Planned | Actual | Difference |
|---|---|---|
| 330 | 283 | 47 |
*The increases of $88.6M from planned spending to total authorities is mainly due to funding for the Canada Health Infoway and for Grants to the Governments of Nunavut, Northwest Territories and Yukon to support the Territorial Health System Sustainability Initiatives.The variance of $8.4M between total authorities and actual spending is largely the result of the reduced requirements in Grant to the Health Council of Canada as well as modest underspending of operating budgets.
**The variance between planned and Actual FTE utilization is mainly due to a change in the planned staffing level during the year.
This program activity provides strategic policy advice on health care issues such as improved access, quality and integration of health care services to better meet the health needs of Canadians, wherever they live or whatever their financial circumstances. The objective is pursued mindful of long-term equity, sustainability and affordability considerations and in close collaboration with provinces and territories, health professionals, administrators, other key stakeholders and citizens.
Improved access, quality and integration of health services administration is achieved through investments in the health system and in health system renewal. These investments support actions such as: reducing wait times for essential services; work with provincial and territorial governments to ensure respect for the principles of the Canada Health Act; development of health information and health measures for Canadians; meeting the health and health access needs of specific groups, such as official language minority communities; and ensuring the implementation of agreements between federal, provincial and territorial ministers of health.
| Performance Indicators |
Targets | Performance Status |
|---|---|---|
| Reports and analyses related to issues such as wait times reduction, health human resources planning, and provision of chronic, palliative and continuing care are used to improve the health care system | Increased awareness and knowledge of new approaches, models and best practices related to health care renewal |
Met All Investments through the Pan-Canadian Health Human Resource Strategy assisted with: increasing the supply of health care providers; using skills effectively; improving workplaces; and effective planning and forecasting. Investments through the Internationally Educated Health Professionals Initiative assisted in development of tools and models for the assessment, bridging and integration of these people into the Canadian health care workforce. Funded palliative and end-of-life care initiatives. |
| Governmental and stakeholder engagement activities (e.g., meetings, workshops, conferences, program and policy proposals) | Increased collaboration and consultation between governments and stakeholders to advance key health care issues |
Met All Support for federal / provincial / territorial eHealth collaboration through funding for Canada Health Infoway. A two year extension of the Territorial Health Systems Sustainability Initiative to support territorial health system reform. A new Health Portfolio wellness approach in all three territories will reduce the administrative burden placed on communities and position community-based programming to better meet the priorities of territories and their communities. Continued to work with the Canadian Institutes of Health Research toward the establishment of the Drug Safety and Effectiveness Network, including staffing, the development of a performance measurement and evaluation framework and contact with international partners implementing related initiatives to share best practices and explore data sharing opportunities. |
| Publication of information that raises awareness and understanding of the factors affecting accessibility, quality and sustainability of Canada's health care system and the health of Canadians | Timely and accessible health research and information on priority health issues available to Canadians |
Met All
The Healthy Canadians 2010 report on health system performance and population health status was enhanced, as recommended by the House of Commons Standing Committee on Health and the Auditor General.
The Health Policy Research Bulletin Health Policy Research Bulletin highlights policy research on themes relevant to the federal Health Portfolio. |
Performance Summary and Lessons Learned
The bulk of work under this program activity related to our ongoing responsibility for policy leadership and research support for health care system improvements. It included our mandate to ensure the principles of the Canada Health Act are respected and to help address the health and health access needs of all Canadians as well as specific groups such as women and official language minority communities.
In addition to those activities, there were areas of particular attention. The department continued to work with provincial, territorial and other partners on major health system sustainability issues. We supported many projects to test actions on Canada's health human resource needs. We also supported an evaluation that determined our Patient Wait Times Guarantee Pilot Project Fund had successfully addressed the Government of Canada priority of informing the establishment of patient wait times guarantees. Provinces and territories intend to move forward with the knowledge gained and with systems and processes from their pilot projects.
To address the shortage of medical isotopes for diagnostic imaging, we worked with the Canadian Agency for Drugs and Technologies in Health. This resulted in an initiative to improve the efficiency and effectiveness in health system management of medical isotopes and alternate medical imaging approaches. We worked with the Public Health Agency of Canada, provinces and territories and others to assess and analyze the response to the 2009 H1N1 outbreak. This included efforts to learn more about patterns of spread and potential counter measures for future situations.
We applied the lessons learned from initiatives to expand the use of electronic health records (EHRs), particularly through the government's support for Canada Health Infoway. The objective that 50% of Canadians would have an EHR available to their authorized health professionals by 2010 was achieved by March 2011. The slight delay reflected different paces of progress among provinces and territories and challenges in encouraging the uptake and adoption of eHealth systems by health professionals. In response, some of the most recent $500 million that Budget 2009 allocated to Canada Health Infoway has focused on the adoption of electronic medical records -- which are currently in 37% of physicians' offices in Canada -- and other eHealth technologies and tools.
Program Activity 2: Canadian Assisted Human Reproduction
Program Activity Descriptions
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 1.3 | 3.4 | 3.4 |
| Planned | Actual | Difference |
|---|---|---|
| 8 | 14 | 6 |
*The variance of $2.1M between Planned Spending and Total Authorities is mainly due to considerations of a broader range of regulatory and legislative options.
**The variance between Planned and Actual FTE Utilization is mainly due to increases in program requirement.
This program activity implements the Assisted Human Reproduction Act, which seeks to protect and promote human health, safety, dignity and human rights in the use of Assisted Human Reproduction (AHR) technologies. It develops policies and regulations to develop a responsive regulatory regime that is a leader both domestically and in the international AHR community, and reflects the objectives put forward in the Assisted Human Reproduction Act. The program activity gathers input from stakeholders, including the provinces, to ensure a pan-Canadian approach. The science of AHR is evolving rapidly. As a result, health and safety are the overriding factors as this program activity engages stakeholders to find a balance between the needs of patients who use these technologies to help them build their families, the children born from these technologies and the providers of these services.
| Performance Indicators |
Targets | Performance Status |
|---|---|---|
| Stakeholder and advisory panel involvement and engagement | Increased stakeholder coordination and consultation on key assisted human reproduction issues to support and advance regulatory development |
Somewhat met
The Department continued to keep in touch with key stakeholders through participation in various committees. No broader consultations took place as the Supreme Court of Canada was assessing the constitutionality of key provisions of the Assisted Human Reproduction Act. |
| Monitoring, collection, and analysis of relevant and current information in assisted human reproduction practices leading to the development of evidence-based policy documents | Improved monitoring and awareness of assisted human reproduction practices leading to an increased number of evidence-based policy documents to support regulatory development |
Mostly met
We collected information related to Assisted Human Reproduction (AHR) practices and stakeholders through means such as a web scan, participation in conferences and communications with AHR specialists. No broader monitoring took place at the Supreme Court of Canada was assessing the constitutionality of the Assisted Human Reproduction Act. |
| Reports and supporting documentation on relevant issues addressed through appropriate regulations and other instruments developed to enforce the Assisted Human Reproduction Act | Assisted Human Reproduction Regulations and other instruments to protect the health, safety, dignity, and rights of Canadians using assisted human reproduction technologies and children born from the use of these technologies |
Not met
The December 22, 2010 decision of the Supreme Court meant that we had to consider new options for moving forward on this issue. |
Performance Summary and Lessons Learned
As planned, our department continued to develop regulatory proposals while we awaited a decision by the Supreme Court of Canada on a challenge to the Assisted Human Reproduction Act. In December 2010, the Court ruled that certain key sections of the Act exceed the legislative authority of the Parliament of Canada, such as those dealing with the licensing and conduct of AHR activities. In response, we began to develop options for a federal role in this field that would reflect the Court's decision.
Program Activity 3: International Health Affairs
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 21.3 | 21.8 | 18.7 |
| Planned | Actual | Difference |
|---|---|---|
| 26 | 30 | 4 |
*The increase of $0.5M from planned spending to total authorities is mainly due to a reduction in the program's required spending profile
**The variance between Planned and Actual FTE Utilization is mainly due to response to emerging international requirements.
Health Canada works internationally through leadership, partnerships and collaboration to fulfill our federal mandate of making Canada's population among the healthiest in the world. We take action to initiate, coordinate and monitor departmental policies, strategies and activities that help promote Canadian priorities and values on the international health agenda. International collaboration on global health issues is important given that the health of Canadians is influenced significantly by public health risks originating in other countries. We address global issues such as pandemic influenza preparedness, HIV/AIDS strategies and global health security with key external health partners such as the World Health Organization (WHO) and the Pan-American Health Organization (PAHO).
Countries and international organizations want to connect quickly to information about Canada's health care system and initiatives. This program activity strives to share Canada's best policies and practices with other countries and assists in the development of bilateral agreements with numerous countries on important health issues. This program activity is the focal point for the delivery of strategic policy advice on international health issues to the Minister of Health, senior management in our department and the Health Portfolio, including representation at international meetings concerning the health portfolio. We also manage grants to non-profit organizations for projects in the domain of international health that are aligned with Canada's priorities in global health.
| Performance Indicators |
Targets | Performance Status |
|---|---|---|
| Strategic engagement with stakeholders and other governments (e.g. consultations and outreach activities with key stakeholders and international partners) | Increased awareness and knowledge of new approaches, models and best practices related to international health priority issues |
Met All Advanced Canada's priorities on issues such as: regulatory cooperation, pandemic influenza preparedness and global health security, through multilateral organizations and other countries. Exchanged information and innovative practices with China on areas of shared interest including chronic disease prevention strategies, emerging and re-emerging infectious diseases, hospital financing, health research, and consumer product safety. |
| Number of new collaborations with key stakeholders on current and emerging inter-national health issues of priority to Canada | Increased strategic engagement in inter-national meetings, conferences and fora; and an increased number of Canadian representatives on the boards or committees of key international health organizations |
Met All Supported and facilitated key high-level international engagement. The 11th Ministerial Meeting of the Global Health Security Initiative focused on lessons learned from the 2009 H1N1 influenza pandemic for future application. The February 2011 Arctic Health Ministers Meeting led to agreement to work collaboratively on circumpolar health issues. We facilitated 8 outgoing and 25 incoming visits from representatives of other countries to share information and best practices about issues such as health care, health system financing and reforms, health human resources, food safety, obesity, eHealth, drug regulations and H1N1. A high-level meeting with Brazilian officials and a policy dialogue with China on shared interests demonstrated our growing attention to the Americas and the Asia-Pacific region. |
| Number of multilateral, bilateral negotiations or agreements that Health Canada leads or supports in order to advance Canada's health priorities | An increase in the number of resolutions or policy positions introduced by Health Canada which reflect Canadian priorities, and policy objectives and an increase in the number of international agreements, treaties or memoranda of understanding which advance Canada's health priorities |
Met All Successful negotiation and passing of resolutions including 28 at WHO, 17 at PAHO and 20 in other United Nations forums. Canadian leadership included sponsorship of resolutions on tobacco control and food safety. Health Canada and PAHO signed a Framework Agreement for Strategic Cooperation for 2011-2012. Negotiations with the Administration for Quality Supervision Inspection and Quarantine (AQSIQ) of China led to a Letter of Intent on cooperation on consumer product safety issues. |
Performance Summary and Lessons Learned
As planned, this program activity continued to centre on Canada's ongoing health-related links with other governments and international organizations. Canada continued to play a critical role in advancing global health policies, in the development of standards and guidelines, and in building global health capacity. We shared information and best practices in areas such as food and consumer product safety and health systems strengthening. We and our international partners paid particular attention to issues that either transcend borders, such as learning from our H1N1 experiences in 2009, or many governments and health systems share, such as how to improve health systems. An ongoing lesson is, that increasingly complex global governance in health, as well as the important health issues and national interests involved, require enhanced effort to improve coordination among all stakeholders.
Strategic Outcome #2
Under this strategic outcome, Health Canada is committed to promoting and protecting the health and safety of Canadians by working towards reducing health risks from health products and food and by providing information so Canadians can make informed decisions and healthy choices.
As the federal authority responsible for the regulation of health products and food, Health Canada evaluates and monitors the safety, quality and efficacy of health products as well as the safety and nutritional quality of food. The Department also promotes the health and well-being of Canadians through a broad range of activities related to health products and food, including developing nutrition policies and standards such as Canada's Food Guide and information to the public in newsletters such as the Canadian Adverse Reaction Newsletter.

Program Activity 1: Health Products
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 144.7 | 176.1 | 170.6 |
| Planned | Actual | Difference |
|---|---|---|
| 1,782 | 1,732 | 50 |
*The increase of $31.4M from planned spending to total authorities is mainly due to incremental funding for review of drug and medical device submissions. The variance of $5.5M between total authorities and actual spending is primarily the result of adjustments to plan related to timing of the passage of the Consumer Products Safety Act.
**The variance between planned and actual FTE utilization is mainly due to adjustments to plan related to timing of the passage of the Consumer Products Safety Act.
The Health Products program activity is responsible for a broad range of health protection and promotion activities that affect the everyday lives of Canadians. Under the authority of the Food and Drugs Act, Consumer Products Safety Act and Regulations, and the Department of Health Act, this program activity evaluates and monitors the safety, quality and effectiveness of drugs (human and animal), biologics, medical devices and natural health products, and conducts surveillance, compliance and enforcement activities. This program activity also provides timely, evidence-based and authoritative information to stakeholders (including but not limited to: health care professionals such as physicians, pharmacists and practitioners such as herbalists, naturopathic doctors and Traditional Chinese Medicine practitioners) and members of the public to enable them to make informed decisions and healthy choices.
| Performance Indicators |
Targets | Performance Status |
|---|---|---|
|
Proportion of regulatory reviews done within service performance standards NDS(New Drug Submission) SNDS(Supplemental New Drug Submission) |
Pharmaceuticals: 90% | New and Supplemental Brand Name (NDS/SNDS) submission reviews Somewhat met - NDS - 73% (59 of 81 decisions) met standard. Mostly met - SNDS - 80% (127 of 159 decisions) met standard. New and Supplemental Generic Drugs (ANDS&SANDS) submission reviews Not met - ANDS -18% (28 of 158 decisions) met standard. Not met - SANDS - 57% (29 of 51 decisions) met standard. |
| Veterinary drugs: 90% | New and Supplemental Brand Name (NDS/SNDS) submission reviews Met all: NDS-90% (9 of 10 decisions) met standard. Exceeded: SNDS-100% (12 of 12 decisions) met & exceeded standard. New and Supplemental Generic Drugs (ANDS&SANDS) submission reviews Exceeded: ANDS-100% (3 of 3 decisions) met & exceeded standard. Exceeded: SANDS-100% (2 of 2 decisions) met & exceeded standard. |
|
| Biologics and Radiopharmaceuticals: 90% | New and Supplemental Brand Name (NDS/SNDS) submission reviews Not met: NDS - 57% (12 of 21 decisions) met standard. Mostly met - SNDS- 80% (66 of 83 decisions) met standard. A temporary backlog related to H1N1 Pandemic was cleared in July 2010 and there has been no backlog in this area since then. Mostly met - NC (Safety) - 86 % met target Met all - NC (Quality) - 92% met target |
|
| Medical devices: 90% | Medical Device application reviews Somewhat met - Class II - 72% 3,763 of 5,182 decisions) met standard. Not met - Class III - 59% (1,332 of 2,250 decisions) met standards. Somewhat met - Class IV - 67% (417 of 621 decisions) met standard. |
|
| Percentage of natural health product pre-market submission backlog completed | 100% addressed by March 31, 2010 100% completed by December 31, 2010 |
Mostly met -99% addressed, with the others halted due to issues that require resolution first. Not rated. This target was superseded under the NHP Unprocessed Product License Application Regulations (UPLAR) that came into force in August 2010. Performance has been between 90% |
| Number of reports on pharmacovigilance plans received (Renamed Risk Management Plans (RMP) and Risk Management Mitigation Plans (RMMP) after publication of the RPP) | Year-over-year increase in pharmacovigilance (Risk Management and Mitigation) plans received | Mostly met RMP Assigned: 38 (56 in 2009-10) RMP Completed: 48 (59 in 2009-10) RMMP Assigned: 32 (6 in 2009-10) RMMP Completed: 20 (3 in 2009-10) |
| Number of pre-submission meetings held per year | Expect to receive 59 pre-submission meeting requests in 2009/10. Anticipate a similar amount in pre-submission meeting requests for biologics and radiopharmaceuticals Expect to receive 125 requests for pre-submission meetings with industry for pharmaceutical drugs |
Met All 40 pre-submission meetings. Responded fully to all industry requests for a meeting. Met All 97 pre-submission meeting requests received. Responded fully to all industry requests for a meeting. |
| Number of Product Monographs made available to the public | In 2010-11, anticipate to have reached an estimated posting of 2000 product monographs on the Health Canada website | Exceeded 1,936 pharmaceutical drug and biologic monographs posted 191 natural health ingredient or product monographs posted 15 Abbreviated Labelling Standards |
| Reduction in prohibited and unapproved heath products entering into Canada | A yearly increase of Health Canada's oversight of imported health products | Not Rated.(first year for this reporting) Total referrals by CBSA - 40,115 Total refused referrals - 30,940 |
| Number of hospitals reporting adverse events | Year-over-year increase in adverse reaction reports from hospitals | Exceeded 2010-11 (as at December 2010) - 1120 AR Reports received from hospitals (approx. 3.4% of total) (981 for same period in 2009-10 / approx. 3.5% of total) 2010-11 (as at December 2010) - 33,956 AR Reports received from all sources, up 23% from previous year, same time) |
| Number of Periodic Safety Update Reports received | Year-by-year increase in Periodic Safety Update Reports received | Exceeded PSUR Assigned: 224 (162 in 2009-10) PSUR Completed: 224 (172 in 2009-10) |
Performance Summary and Lessons Learned
In addition to our mandated responsibilities, we focused on implementing the aspects of the Food and Consumer Safety Action Plan that were within our existing regulatory framework. While we were largely successful in reaching many of our performance targets, we developed backlogs in the review of new human pharmaceutical and medical device submissions due to larger than expected volumes. We believe that the implementation of cost recovery in April 2011 will help us to meet our performance targets and achieve financial stability.
Enhanced collaboration and outreach were key elements in the year's work under this program activity. We worked with a range of partners on how best to maintain Canada's position as a global leader in the emerging field of cell therapies. We also met with industry representatives to communicate and collaborate on specific vaccine regulatory issues. This collaborative approach is increasingly international in scope. For example, we worked with our American and World Health Organization counterparts to exchange knowledge and experience gained in vaccine release and immunization around the world throughout the 2009 influenza pandemic. We increased our use of data from foreign regulatory agencies, particularly those in the United States and the European Union, to improve access to veterinary drugs for Canadian producers.
Our departmental regulatory branches worked towards the development of a regulatory framework through regulatory and non-regulatory measures to address areas of concern under the Food and Drugs Act. We also moved toward improved consistency and flexibility in our regulatory activities through work on a standard model and a more risk-based approach within and across our regulatory responsibilities.
We responded to the rising number of new generic pharmaceuticals being submitted for approval by mapping our processes to identify areas where streamlining would be possible. We have been successful in reducing backlogs in medical device applications by improving workflows and eliminating processes that do not add sufficient value. Our increasing engagement with industry and professional groups and our availability for meetings prior to submissions has been beneficial in increasing awareness of scientific issues and our regulatory requirements.
Program Activity 2: Food and Nutrition
The Food and Nutrition program activity establishes policies, regulations and standards related to the safety and nutritional quality of food. Food safety standards are enforced by the Canadian Food Inspection Agency. The legislative framework for food is found in the Food and Drugs Act and Regulations, the Canadian Food Inspection Agency Act and the Department of Health Act. The program activity also promotes the nutritional health and well-being of Canadians by collaboratively defining, promoting and implementing evidence-based nutrition policies and standards. As the focal point and authoritative source for nutrition and healthy eating policy and promotion, the program activity disseminates timely, evidence-based and authoritative information to Canadians and stakeholders to enable them to make informed decisions and healthy choices.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 69.7 | 70.6 | 58.4 |
| Planned | Actual | Difference |
|---|---|---|
| 603 | 465 | 138 |
*The variance of $0.9M from planned spending to total authorities is mainly due to a fund transfer from Agriculture and Agri-Food Canada to address innovation and industry advance issues identified by the the agriculture and agri-food sector, as part of the Agriculture Regulatory Action Plan. The variance of $12.2M between total authorities and actual spending is mainly due to adjustments to plan related to timing of the passage of the Consumer Products Safety Act.
**The variance between Planned and Actual FTE utilization is mainly due to adjustments to plan related to timing of the passage of the Consumer Products Safety Act.
| Performance Indicators |
Targets | Performance Status |
|---|---|---|
| Level of Stakeholder and Public Awareness | Health Canada anticipates distributing over 3,500,000 copies of Eating Well with Canada's Food Guide (English and French), over 1,200,000 visits to the Food Guide main page and over 350,000 visits to the My Food Guide online web page | Mostly met 3.1 million copies of Canada's Food Guide distributed 1.23 million visitors to the main Food Guide website 359,000 personalized PDF files created with My Food Guide |
| Efforts to increase consumer awareness of the Nutrition Label will continue and in 2010-11, Health Canada anticipates over 5,000 visitors using the Interactive Nutrition Labelling Quiz | The Nutrition Facts Education Campaign was launched 4500 respondents completed the Interactive Nutrition Labelling Quiz |
|
| Health Canada will continue to strengthen capacity building by interpreting and sharing results from the Canadian Community Health Survey 2.2, Nutrition Focus | New information posted on nutrient intakes of Canadians and current statistics on breastfeeding practices and household food insecurity Redesign of the web pages and new graphics, facilitate easy access to trends and data |
|
| Health Canada will establish a Food Regulatory Advisory Committee that will provide broad expert strategic policy advice on the safety of food products and will be composed of repre-sentatives from key stakeholder groups Publish a report summarizing the input received during the stakeholder consultations on the enhancement of precautionary labelling of allergens in food |
Inaugural meeting of the Food Regulatory Advisory Committee held in September 2010 Regulatory amendments related to "Enhancing labelling for food allergens, gluten sources and added sulphites" were published in February 2011 |
|
| Number of educational tools developed |
Health Canada will also develop and disseminate education tools:
|
Met all We published guidance on our website in early 2010 New resources included a background document and handout for health professionals and an on-line interactive tool for consumers New content was published on the HC website in 2010/2011 Produce Safety New guidance published on HC website in early 2010 Preparing and Handling Powdered Infant Formula In 2010-11, Health Canada released resources on healthy weight gain in pregnancy, including a background document and handout for health professionals and an on-line interactive tool for consumers. |
| Proportion of Health Risk Assessments(HRA) for acute health risks communicated to stakeholders within service standards (as part of the Rapid Response pillar of the Food and Consumer Safety Action Plan) | 90% within 24-48 hours | Exceeded 100% of HRAs were conducted within time standards |
| Proportion of Health Risk Assessments related to health risks of lesser severity communicated to stakeholders within service standards (as part of the Rapid Response pillar of the Food and Consumer Safety Action Plan) | 90% within 5-10 days | Exceeded 100% of HRAs were conducted within time standards |
Performance Summary and Lessons Learned
In addition to our ongoing responsibilities to tackle food safety issues and inform Canadians about what they eat and how to handle food safely, Listeria, sodium, trans-fats and caffeine were the focus of Parliamentary and public attention during 2010-2011. Our department made substantial progress in addressing the contamination of ready-to-eat (RTE) foods by the microorganism Listeria monocytogenes. For example, a new policy was published, as well as the most comprehensive set of requirements developed by a food regulatory agency to enhance the control of this microorganism during the processing of RTE foods. We reviewed and validated rapid methods to test Listeria monocytogenes in the environment and in finished products. The department also reviewed and approved two high pressure treatment processes and a new food additive, micocin, to reduce microbial contamination of foods.
Health Canada moved forward on issues related to sodium. Health Canada has been working to establish sodium reduction targets for foods sold in Canada. Federal , Provincial and Territory Ministers of Health have endorsed a target to reduce the average consumption of sodium to 2300 mg/day by 2016. We also developed draft messages for public education materials for testing with consumers and intermediaries, and hosted a joint World Health Organization-Canada Exchange Forum and Technical Meeting on Sodium Surveillance, Monitoring and Evaluation.
The profile and importance of food safety issues has meant that we have to be flexible with our resource allocations and we need to ensure that we have the facilities and skilled people needed to meet our needs. We are also underlining the value of working with our counterparts in other countries.
Strategic Outcome #3
Health Canada is responsible for assessing and acting on many elements of day-to-day living that have impacts on the health of Canadians. These include drinking water safety, air quality, radiation exposure, substance use and abuse (including alcohol), consumer product safety, tobacco and second-hand smoke, workplace health, and chemicals in the workplace and in the environment. The Department is also engaged in chemical and nuclear emergency preparedness, inspection of food and potable water for the travelling public and health contingency planning for visiting dignitaries.
Much of this work is governed by legislation such as the Controlled Drugs and Substances Act, the Hazardous Products Act, the Tobacco Act, the Food and Drugs Act, the Radiation Emitting Devices Act, the Quarantine Act, the Pest Control Products Act and others.
Program Activity 1: Sustainable Environmental Health
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 152.2 | 141.1 | 134.9 |
| Planned | Actual | Difference |
|---|---|---|
| 828 | 852 | 24 |
*The decrease of $11.1M from planned spending to total authorities is mainly due to decrease in program requirements.
**FTE utilization variance is primarily attributable to project /activity changes.
Environmental factors continue to be a key determinant of health for all Canadians. Canadians benefit from this program activity, which promotes and protects the health of Canadians by identifying, assessing and managing health risks posed by environmental factors in living, working and recreational environments. The scope of activities includes: research on drinking water quality, air quality, contaminated sites, toxicology and climate change. It extends to clean air programming and regulatory activities as well as the risk assessment and management of new and existing substances, air pollutants, environmental noise, environmental electromagnetic frequencies, products of biotechnology and products of other new and emerging technologies (including nanotechnology). Other matters under this program activity include issues related to solar ultraviolet radiation; preparedness for nuclear, radio-nuclear, chemical and biological incidents as well as working with the passenger conveyance industry (e.g., airlines, cruise ship operators and passenger railway companies) to protect the travelling public.
Under the Sustainable Environmental Health program activity, Health Canada delivers on the Government of Canada's Chemicals Management Plan (CMP) by assessing the health risks of and developing risk management strategies for new and existing substances that enter the environment through manufacturing, use in consumer products or their disposal. Key initiatives under the CMP that support this program activity include: implementing a national system to track actual exposures to potentially harmful chemicals; ensuring that Canadians have laws and standards and information about the health risks of chemical substances to protect them from risks of potentially harmful chemicals, as well as precautions Canadians can take to protect their health; and working with industry sectors to develop comprehensive risk management practices. Under this program activity, Health Canada also works to protect the health of Canadians by working with other jurisdictions in improving air quality and safe drinking water. For example, Health Canada works with Environment Canada, provinces and territories on a national framework to manage air pollution, in collaboration with industry and non-governmental organizations.
| Performance Indicators |
Targets | Performance Status |
|---|---|---|
| Proportion of regulatory activities addressed within service standards/target | These baselines are being established as part of the renewal processes in 2011 for a number of environmental health initiatives | Not rated as baseline being established in 2011 |
| Time period within which serious health risks are brought into a risk management regime | Not rated as baseline being established in 2011 | |
| Percentage of the target population aware of environmental health issues | Not rated as baseline being established in 2011 |
Performance Summary and Lessons Learned
Health Canada responsibilities under the Government's environmental commitments to Canadians were a major emphasis of this program activity in 2010-2011. Under the Chemicals Management Plan, our Department has been assessing the health risks of new and existing chemicals and has developed risk management strategies where needed. We also responded to stakeholder inquiries and added to the awareness of Canadians about what they can do to reduce risks. Recognizing the link between air quality and health, the Department continued to support the Government's Clean Air Agenda. We expanded the Air Quality Health Index (AQHI) to more communities in 2010-11, for a total of 49 locations making the AQHI available to more than half of all Canadians. Our department worked with the Public Health Agency of Canada on the Drinking Water Advisory Module. This notification and information-sharing tool for public health and drinking water authorities captures key information on Canadian drinking water advisories. It permits analyses and reporting on key trends and root causes of advisories across Canada.
As with many Health Canada responsibilities, this program activity is a focal point for emergency responses. When the March 2011 earthquake in Japan triggered a nuclear emergency, we increased our monitoring capacity in British Columbia and regularly posted data on our website to inform Canadians. In collaboration with other partners, we provided daily advice to the Department of Foreign Affairs and International Trade and the Canadian Embassy in Japan, and we supplied environmental and personal monitoring equipment to the Canadian Foreign Mission in Tokyo and to Province of B.C. Within Canada, we provided guidance to airline and marine industry operators on environmental decontamination, water quality and border screening issues.
Our experience and that of other departments with the first phase of the Chemicals Management Plan have all been factored into government-wide thinking about the planned policies, programs and processes that could be part of a possible next phase of the Chemicals Management Plan. We have seen opportunities for greater efficiencies and improvements in risk management strategies. We have shared our lessons learned with other countries to inform global decision-making on the assessment and management of chemicals, and have also learned from the experiences of other countries.
Program Activity 2: Consumer Products
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 33.9 | 33.6 | 27.9 |
| Planned | Actual | Difference |
|---|---|---|
| 265 | 120 | 145 |
*The decrease of $0.3M from planned spending to total authorities is mainly due to decrease in program requirements.
**The variance of $5.7M between total authorities and actual spending and the FTE utilization variance are primarily attributable to adjustments to plan related to timing of the passage of the Consumer Products Safety Act.
Health Canada identifies, assesses, manages and communicates to Canadians the health and safety risks associated with consumer products (those products that adults and children commonly use for personal, family, household and garden use or use in recreational and sports activities). The benefit of this program activity is that actions taken minimize the risks that consumer products may pose to Canadians. We achieved this through compliance and enforcement actions, consumer and industry outreach activities and surveillance and risk assessment work. The acts that guide our work include: Hazardous Products Act (consumer products) and Food and Drugs Act (cosmetics regulations) and the Radiation Emitting Devices Act.
| Performance Indicators |
Targets | Performance Status |
|---|---|---|
| Percentage of inspected registrants/firms / users who are compliant / non-compliant with product safety obligations | Corrective action taken on 100% of non-compliant products inspected identified through targeted cyclical enforcement plan | Met All The 2010-2011 cycle targeted 13 product categories with hazards and baseline data (as identified in previous cycles). Corrective action was taken on 100% of non-compliant cases (e.g., recalls, industry communication, stop-sales, education and industry commitments) |
| Number of incidents reported of improper/unsafe use of consumer products | Year-over-year decreasing trend in number of reported incidents measured against baseline data to be established in 2010 | Not Rated Establishment of a baseline was not possible in fiscal year 2010-11, as the Canada Consumer Product Safety Act, including the provision for mandatory incident reporting, came into force June 20, 2011. The baseline will be established by early 2013. It is also important to note that the targeted year-over-year decreasing trend in number of incidents reported will be preceded by an increase in the number of incidents as industry comes into compliance with the new mandatory incident reporting requirements. |
| Percentage of issues addressed under product safety legislation and its regulations | Year-over-year improvement in the number of issues addressed. Targeting 100% of issues addressed by 2014 | Not Rated Establishment of a baseline was not possible in fiscal year 2010-11, as the Canada Consumer Product Safety Act, including the provision for mandatory incident reporting, ,came into force June 20, 2011. |
Performance Summary and Lessons Learned
Health Canada's Consumer Products Program Activity continued to ensure that consumer products were as safe as possible. We addressed consumer product risks and concerns through ongoing targeted inspections, surveillance and compliance promotion (both domestically and internationally) under the Hazardous Products Act. The program activity also supported outreach activities to Canadians on the potential dangers associated with some consumer products.
We adjusted our planning under this program activity for 2010-2011 to align with the passage of and Royal Assent to the Canada Consumer Product Safety Act. Accordingly, we worked under the regulatory framework of the Hazardous Products Act. Both acts mandate post-market surveillance. The sampling for compliance is targeted to those product categories where there is a reasonable assumption of non-compliance (i.e., higher risk products) and takes place according to a planned cycle. During 2010-2011, we inspected 13 categories of products, including carpets, cribs and cradles, tents and cosmetics. That work complemented our ongoing inspection and enforcement activities in response to consumer complaints (which have risen each year from an initial 567 in 2006-07 to 1359 in 2010-2011) and incident reports, referrals from other organizations and other initiatives.
We also continued to act on specific health and safety issues. New regulations were announced restricting the use of phthalates in children's toys and child care articles and lead in children's products. Regulations were updated for cribs, cradles and bassinets to further strengthen Canada's safety requirements, and for surface coating materials to lower the acceptable limit for lead. Enforcement actions under our cyclical enforcement projects resulted in 35 recalls. We posted 287 product recalls for 2010-11. To support this activity, we implemented a recall effectiveness form for industry to improve recall efficiency and monitoring.
Program Activity 3: Workplace Health
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 20.2 | 31.7 | 31.7 |
| Planned | Actual | Difference |
|---|---|---|
| 331 | 274 | 57 |
*The increase of $11.5M from planned spending to total authorities is mainly due to funding for the organization of the 2010 G8 / G20 Summit.
**The variance between planned and actual FTE utilization is mainly due to internal reorganization and related issues.
This program activity provides services to protect the health and safety of the federal public sector, visiting dignitaries, and others. Specific programs include: the provision of occupational health services to federal employees; delivery of the Employee Assistance Program; emergency health services to Internationally Protected Persons; dosimetry services (the measurement of personal, occupational exposure to radiation through the reading of "dosimeters" or plaques enclosed in special holders worn by the user for specified periods); and the Workplace Hazardous Materials Information System, which is a national hazard communication standard that includes worker education, inspector training and standards for cautionary labels.
| Performance Indicators |
Targets | Performance Status |
|---|---|---|
| Percentage of public service employee clients' psycho-social problems dealt with within service standards | 70% (represents the current Industry standard) | Exceeded More than 90% of cases were dealt with within the short-term, solution-focused approach of our Employee Assistance Program |
| Percentage of visits/events without serious health related incidents for Internationally Protected Persons or for Canadian Public Servants | 100% | Met All There were no serious health-related incidents for Internationally Protected Persons (IPPs) in the 40 IPP regular visits and eight high-level visits that required dedicated ambulance and food surveillance services |
Performance Summary and Lessons Learned
Of note in our ongoing requirement to supply health and medical services to Internationally Protected Persons was our involvement in the G8 and G20 Summits with a focus on the needs of the participating Heads of State and/or Governments and their immediate family members as well as RCMP officers and all staff on-site. We also provided services for the Royal Visit of Her Majesty the Queen and the visits of Princess Anne and Prince Andrew, which were successful due to tailored contingency health plans. We also pursued emergency preparedness as needed throughout our department and with Health Portfolio organizations and put measures in place to ensure that regulatory activities can respond to a pandemic threat. After the heavy involvement in the 2010 Olympic and Paralympic Winter Games, as well as deployment during the G8 and G20 Summits, we intend to review how we can improve our service delivery performance and efficiency during major events.
Program Activity 4: Substance Use and Abuse
Through regulatory, programming and educational activities, Health Canada seeks to improve health outcomes by reducing and preventing tobacco consumption and addressing alcohol and drug abuse. Through the Tobacco Act and its regulations, along with the new Cracking Down on Tobacco Marketing Aimed at Youth Act, Health Canada regulates the manufacture, sale, labelling, and promotion of tobacco products. We also lead the Federal Tobacco Control Strategy that aims to: further reduce the prevalence of smoking; reduce exposure to second hand smoke; and, reduce death and disease caused by smoking.
Health Canada administers the Controlled Drugs and Substances Act and its regulations. Through four regional labs, we provide expert scientific advice and drug analysis services to law enforcement agencies. The Marihuana Medical Access Regulations control the authorization for use and cultivation of marihuana by those suffering from grave and debilitating illnesses. Our department is a partner in the government's National Anti-Drug Strategy. It includes: prevention programming aimed at youth; facilitating access to treatment programs; compliance and enforcement activities related to controlled substances and precursor chemicals; and, increased resources to the Drug Analysis Service to support the increase in law enforcement resources.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 133.6 | 140.8 | 124.0 |
| Planned | Actual | Difference |
|---|---|---|
| 465 | 415 | 50 |
*The increase of $7.2M from planned spending to total authorities is mainly due to incremental funding to support the defence of Canada in tobacco litigation. The variance of $16.8M between total authorities and actual spending is primarily the result of delayed requirements in the Drug Treatment Funding Program and timing of legislation related to the National Anti-Drug Strategy.
**The variance between planned and actual FTE utilization is mainly due to staffing issues related to the Medical Marijuana Access Program which switched to the use of temporary help for carrying out some required activities.
| Performance Indicators |
Targets | Performance Status |
|---|---|---|
| Smoking prevalence rate in % of the Canadian Population | 12% (Canadian Tobacco Use Monitoring Survey) |
Not met Prevalence (%) of smoking amongst Canadians aged 15 years or older in 2008 and 2009:
|
| Prevalence rates of drug use and abuse | To be set after baseline is established in 2010-11 |
Not rated Prevalence (%) of drug use (past year) among Canadians (15+) in 2008 and 2009:
|
| Number/nature of injuries and/or environmental risk caused by unsafe handling of chemicals noted by Drug Analysis Service personnel | Zero injuries | Mostly met One minor injury reported during clandestine laboratory dismantlement |
| Rates of compliance with policies and regulations | 95% compliance Cigarette Ignition Propensity (CIP)IP 100% compliance Labelling (Tobacco) 100% compliance Sales to Youth 100% compliance to the new Cracking Down on Tobacco Marketing Aimed at Youth Act (2009) |
Mostly met Compliance rate by type of tobacco inspection:
Non-compliant products were seized due to contraventions of minimum packaging requirements or the suspected presence of prohibited additives. 4 warning letters were sent to manufacturers for packages of little cigar products with less than the minimum 20 units. * Federal inspections on sales to youth are limited to Alberta and Saskatchewan. |
| Level of awareness about harmful health and social effects associated with illicit drug use | Year over year level of increase in awareness about the harmful health and social effects associated with illicit drug use. Baseline = 2009 |
Met all Between 2009 and 2010, increased youth awareness about the harmful effects of illicit drug use Survey comparisons show that for youth:
|
| Extent to which the Drug Treatment Funding Program (DTFP) has contributed to and strengthened, evidence-informed substance abuse treatment systems and services | Based on the baseline information collected in 2010- 2011, target to be set in 2011-2012 | Not rated DTFP provided funding to 29 treatment systems and services projects up to March 31, 2011. Evidence is starting to emerge that project recipients are demonstrating increased collaboration within and across jurisdictions, and health systems are delivering enhanced treatment services with focus on the needs of at-risk youth. |
Performance Summary and Lessons Learned
Since 2001, this program activity has resulted in a reduction in smoking uptake among Canadian youth; an increase in the number of Canadians who quit smoking and a reduction in the number of Canadians exposed daily to second-hand smoke. However, there has been no decline is smoking prevalence since 2005, and just under five million Canadians still continue to smoke. Health Canada also pursued its work in relation to illicit drug use. For example, we conducted 101 Precursor Control Regulation (PCR) inspections and 40 Controlled Drugs and Substances (CDS) inspections.
Program Activity 5: Pesticide Regulation
To help prevent unacceptable risks to people and the environment, and facilitate access to sustainable pest management tools, Health Canada, through the Pest Management Regulatory Agency, regulates the importation, sale and use of pesticides under the federal authority of the Pest Control Products Act and its Regulations.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 47.0 | 50.7 | 46.3 |
| Planned | Actual | Difference |
|---|---|---|
| 588 | 513 | 75 |
*The increase of $3.7M from planned spending and total authorities is mainly due to a transfer from Agriculture and Agri-Food Canada to address innovation and industry advance issues identified by the agriculture and agri-food sector, as part of the Agriculture Regulatory Action Plan. The variance of $4.4M between total authorities and actual spending is mainly due to increase in cost recovery
**The variance between planned and actual FTE utilization is mainly due to staffing restriction measures implemented during the fiscal year in relation to sunsetting initiatives.
| Performance Indicators |
Targets | Performance Status |
|---|---|---|
| Pre-market reviews and regulatory decisions on new pesticide products and new uses of pesticide products completed within performance timelines that meet international standards | 90% of reviews completed within performance timeline targets |
Mostly Met Category A = 82% (72 of 88) Category B = 80% (369 of 464) Category C = 74% (860 of 1162) Category A--submission to register a new active ingredient (not yet registered in Canada) and associated end use products, or to amend the registration of a currently registered product by adding a major new use which requires an extensive data review and risk assessment |
| Re-evaluation assessments completed within commitments under the Chemicals Management Action Plan | 90% of older registered pest control products have undergone a full review in the last 15 years |
Met All 93% of assessments completed within performance standards (373 of 401 active ingredients)
|
| Delivery of the National Pesticides Compliance Program including associated investigations/ enforcement responses | 80% of compliance programs and enforcement activities delivered and reported according to timelines | Exceeded Inspections = 99% (973 of 986) Investigations = 91% (594 of 653) Analysis and reports = 80% (150 of 188) Enforcement responses = 1157 (e.g., seized, denied entry, aimed at correcting the non-compliance) |
| Development of new transition strategies to use of lower risk pesticides | Increased availability of reduced risk and low risk pesticide products |
Met All 29 non-conventional and microbial category A reviews were completed Microbials A are microorganisms (such as bacteria and fungi) that are used as the pest control agent . Non-conventional pesticides are naturally occurring substances. |
Performance Summary and Lessons Learned
Through the Pesticide Regulation program activity, we continued our ongoing responsibilities under the Pest Control Products Act and supported the re-evaluation of pesticides as part of the Chemicals Management Plan. These approaches were consistent with our overall commitment to modernize our safety framework. They included achievements such as the elimination of backlogs of applications in some categories. Collaboration with international partners is a growing element of our results in this program activity. International sharing of review information is enabling Canada to benefit from standardized global approaches to risk assessment processes. There were 31 international joint review requests in 2010-2011, compared to 27 for the previous three fiscal years together. We led development of an innovative Organization for Economic Co-operation and Development (OECD) regulatory test guideline that is among the largest recent transformations of regulatory toxicology.
Our department implemented new regulations that respond to market needs by encouraging the registration of new, innovative pesticides and facilitating the timely entry of competitively priced generic pesticides. We also implemented new risk mitigation measures for rodenticides to protect children, pets and non-target species. Funding under the Food and Consumer Safety Action Plan enabled us to deliver programs and projects. One example was a partnership that helped cut non-compliance related to aquaculture. Under our Outreach program, we targeted 'Read the Label' campaigns on flea and tick products. We enhanced public access to information and tools with a new web based tool to promote best application practices.
We faced a challenge in our ability to meet demands for reviews of fungicides. Shortened time lines had been negotiated, which combined with somewhat limited expertise to affect our ability to meet performance standards. We had to redirect resources from assessing other submissions which affected those performance standard results. Both situations underline the ongoing need to identify and act on program priorities.
Strategic Outcome #4
Health Canada delivers or funds a range of health programs and services to First Nations and Inuit. A range of primary care services are provided in approximately 200 First Nations communities, largely in rural or remote areas where access to provincial health care services is limited. In addition, home and community care services are provided in approximately 600 First Nations communities. Health Canada supports a range of community-based health programs, focusing on children and youth, mental health and addictions, and chronic disease and injury prevention. Our Department also supports a range of public health programs with a focus on control of communicable diseases (e.g., tuberculosis, HIV/AIDS and vaccine-preventable diseases), environmental public health (e.g., public health inspections and monitoring drinking water quality) and research. The Non-Insured Health Benefits Program provides more than 800,000 eligible First Nations people and Inuit with a limited range of medically necessary health-related goods and services not provided through private insurance plans, provincial/territorial health or social programs or other publicly funded programs.

Program Activity 1: First Nations and Inuit Health Programming and Services
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 2,199.7 | 2,440.8 | 2,402.1 |
| Planned | Actual | Difference |
|---|---|---|
| 1,867 | 2,463 | 596 |
*The increase of $241.1M from planned spending to total authorities is mainly due to renewal of the Federal Aboriginal Health Programs, the continued implementation of the Indian Residential Schools Settlement Agreement, and the extension of the First Nations Water and Waste Water Action Plan. The variance of $38.7M between total authorities and actual spending is mainly due to the reprofile of funding for the National First Nations Public Health Surveillance projects to future years and the return of $8.0M in the Non- Insured Health Benefits Program funds for Qalipu (Newfoundland Landless Indians)
**The variance between planned and actual FTE utilization is mainly due to increases in program funding and related staffing.
The provision of health programs and services by Health Canada to First Nations and Inuit is rooted in the Federal Indian Health Policy. The Department provides health programs and services to First Nations and Inuit as a matter of policy, using annual Appropriations Acts to obtain Parliamentary approval. Through our regional offices and together with First Nations, Inuit and other health partners, we support public health and community health programs that benefit on-reserve First Nations and Inuit directly. These include environmental health and communicable and non-communicable disease prevention, and provision of primary health care services through nursing stations and community health centres in remote or isolated communities to supplement and support the services that provincial, territorial and regional health authorities provide. The Department also supports targeted health promotion programs for Aboriginal people, regardless of residency as well as counselling, addictions and mental wellness services. The Non-Insured Health Benefits coverage of drug, dental care, vision care, medical supplies and equipment, short-term crisis intervention mental health services, and medical transportation is available to all eligible First Nations and Inuit in Canada, regardless of residency.
| Performance Indicators |
Targets | Performance Status |
|---|---|---|
| Life expectancy (at birth by gender, on and off reserve), comparison of First Nations and Inuit with other Canadians Birth weight (comparison of First Nations and Inuit with other Canadians) Infant mortality rates (comparison of First Nations with other Canadians) Rates of conditions by type--e.g., diabetes, suicide |
Food security pilot projects implemented in two First Nations and Inuit communities | Exceeded Seven pilot projects were implemented |
| 90% of First Nations communities with a tested pandemic preparedness and response plan | Met All 98% of First Nations communities have developed a pandemic plan and 87% have tested components of their pandemic plan |
|
| 200 sites have access to telehealth services | Met All 200 sites have access to telehealth services |
|
| Accreditation of three Native Alcohol and Drug Abuse Treatment Centres | Exceeded Six Centres were accredited |
|
| Certification of 100 additional addictions workers in the next two years | Met All 50 certified addictions workers in year one |
|
| 200 First Nations and Inuit youth suicide prevention projects implemented | Mostly All 173 projects supported |
|
| 80 maternal child health projects implemented in 200 communities | Exceeded 125 projects in 225 communities |
|
| 600 First Nations communities with diabetes prevention services | Met All Services in over 600 communities |
Performance Summary and Lessons Learned
As expected, while the vast majority of expenditures under this program activity involved ongoing departmental programs and services for First Nations and Inuit health, our department took action to follow through on the significant federal government commitments to Aboriginal health in recent Speeches from the Throne and Budgets. For example, we drew on the Budget 2010 commitment of $730M over five years to support programming in fields such as targeted health promotion and disease prevention. These include the Aboriginal Diabetes Initiative; the Maternal Child Health Program; Aboriginal Head Start On Reserve; the National Aboriginal Youth Suicide Prevention Strategy; the Aboriginal Health Human Resources Initiative; and, the Health Service Integration Fund (formerly the Aboriginal Health Transition Fund). The regional operations of our department are actively engaged infection prevention and control (IPC) activities with communities in their regions under a new IPC Strategy that we developed in 2010-2011.
In British Columbia, we finalized a 10-year Tripartite Health Plan with the provincial government and First Nations representatives. It establishes a long-term strategy for improving First Nations health programs and services and supports the development of individual First Nation health plans. The Health Plan recognizes the importance of community solutions and approaches. In Saskatchewan, progress was made toward a First Nations Health and Wellness Plan. Once ratified, the Wellness Plan will lead to increased integration, coordination and harmonization of health programs and services.
The department and our partners in all levels of government, including on-reserve First Nation communities, achieved improved levels of preparedness by applying lessons learned during the 2009 H1N1 pandemic. Our department continued to implement the Budget 2009 commitment under Canada's Economic Action Plan of $457.7 million over two years. We used the funds to complete approximately 40 new major health facility infrastructure projects and approximately 135 minor renovation projects. To address individual project delays and rising project costs and within a fixed budget, we had to delay some minor renovations that had been initially planned to begin in 2010-11. In addition to commitments that we set out in our Report on Plans and Priorities, we also supported the introduction of the proposed Safe Drinking Water for First Nations Act (Bill S-11) that was still under review when Parliament was dissolved for the general election.
Evaluation results of our programming enable us to make improvements when we design and deliver later generations of similar programs and services. For example, we drew on the evaluation of the Aboriginal Health Transition Fund (AHTF) to develop the new Health Services Integration Fund (HSIF). Like AHTF, the new HSIF will emphasize the importance of Aboriginal engagement in program design, delivery and priority setting, the importance of sound governance structures and the recognition that progress in Aboriginal health services takes time, dedicated resources and an understanding of system complexities.
Program Activity 2: Internal Services
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 327.6 | 363.1 | 357.1 |
| Planned | Actual | Difference |
|---|---|---|
| 2,652 | 2,604 | 48 |
*The variance of $35.5M between Planned Spending and Total Authorities is mainly due to funding related to corporate support to Federal Aboriginal Health Programs. The variance of $6.0M between Total Authorities and Actual Spending is mainly due to the implementation of a cost containment strategy, a more strategic staffing approach, as well as increased efficiencies associated with IT and ATIP projects.
**The variance between Planned and Actual FTE Utilization is mainly due to some staffing delays, combined with the unexpected departure of employees due to work relocation.
Performance Summary and Lessons Learned
In the Report on Plans and Priorities, we identified initiatives addressing key departmental internal service advances, designed to help deliver on the management priorities set out in Section 1 of this report. This program activity also includes the ongoing departmental commitment to supporting sustainable development and incorporating it into Health Canada planning and activities.
As committed, we made progress on our Strategic Policy Renewal initiative. Specific deliverables included confirmation of priorities in our Medium and Longer Term Policy Agenda, improved scanning of our policy environment, employee development activities and finalization of a new Health Portfolio Strategic Policy Framework. These and other initiatives contributed to an improved basis for policy advice to the Minister and senior management, stronger policy capacity in Health Canada, and a more collaborative work culture across the Department.
We also developed a Science Plan that focuses on the development of science priorities; a science excellence framework; laboratory infrastructure renewal; improved linkages between our science and policy functions; and science and technology talent management. The Science Plan began to generate results through measures such as a Laboratory Infrastructure Renewal Plan, through which we have improved laboratory conditions. It also led to research policies on issues such as scientific integrity, scientific publications and intellectual property, and a Talent Management Strategy to guide our efforts to attract and retain scientific expertise.
In order to better align HR services and practices to the current business goals and talent needs of the Department, we made progress in implementing our overall Talent Management Strategy. This involved a new Health Canada Learning Strategy that fosters the learning culture that should help us to attract, develop, engage and retain the kind of people we need to deliver results. We also launched a new approach to official language training that improves management and results in this area. Web 2.0 was successfully implemented in support of the Department's business processes for information sharing, interoperability, and collaboration. Health Canada demonstrated continued improvement in corporate planning, accountability and reporting processes. A new Program Activity Architecture was developed and implemented for the 2011-2012 fiscal year, supported by improved performance measurement indicators. A stronger Financial Management Control Framework was complemented by the launch of a mandatory Agreement/Recipient Risk Assessment Tool for managing risks in order to improve management of our grants and contributions programming.
Our department reorganized our regional operations to create an environment that allows programs with similar functions to work horizontally. This will help us achieve more integrated, aligned and consistent program delivery to Canadians and generate better results in areas such as compliance and enforcement, as well as in our prevention, promotion and health risk reduction programming and in our laboratory management functions.
Consistent with our commitment to increase departmental transparency and engagement with Canadians, we implemented communications process improvements and new policies. This helped as we enhanced our use of social media through a successful pilot project developing YouTube videos on selected topics, with a particular focus on risk. The videos delivered information to new audiences and complemented traditional communications practices.
Health Canada continued to support the Government of Canada's commitment to sustainable development under the Federal Sustainable Development Act through the integration of the Departmental Sustainable Development Strategy into the operational planning process and as part of the Report on Plans and Priorities in March 2011.
Section III: Supplementary Information
Financial Highlights
| % Change | 2010-11 | 2009-10 | |
|---|---|---|---|
| Total Assets | -10% | 477,701 | 530,507 |
| Total Liabilities | -12% | 1,111,273 | 1,256,282 |
| Equity of Canada | -13% | (633,572) | (725,775) |
| Total | -10% | $477,701 | $530,507 |
| % Change | 2010-11 | 2009-10 | |
|---|---|---|---|
| Total Expenses | -11% | 3,815,675 | 4,306,900 |
| Total Revenues | 7% | 90,965 | 84,969 |
| Net Cost of Operations | -12% | $3,724,710 | $4,221,931 |
Assets by Type
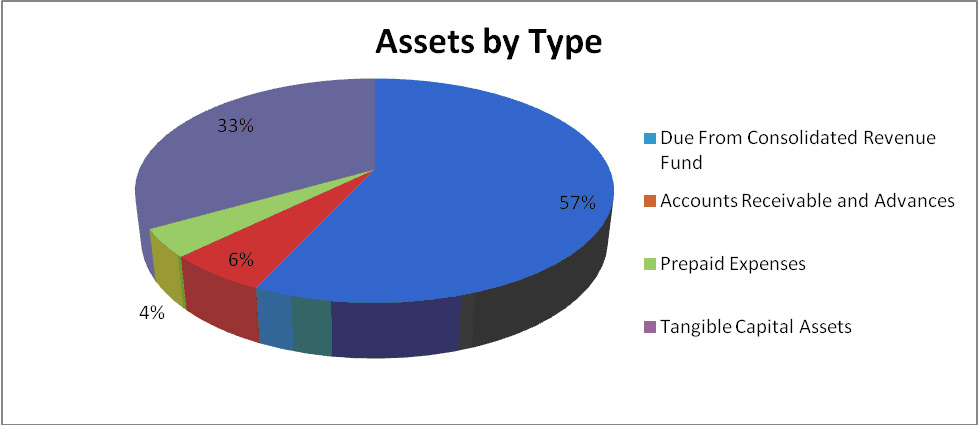
Total assets were $477.7M at the end of 2010-11, a decrease of $52.8M from the previous year. The majority of the change was due to a decrease in the Due from the Consolidated Revenue Fund account of $58.6M. These were offset by increases in Capital Assets $1.9M and Prepaid Expenses $4.2M.
Liabilities by Type
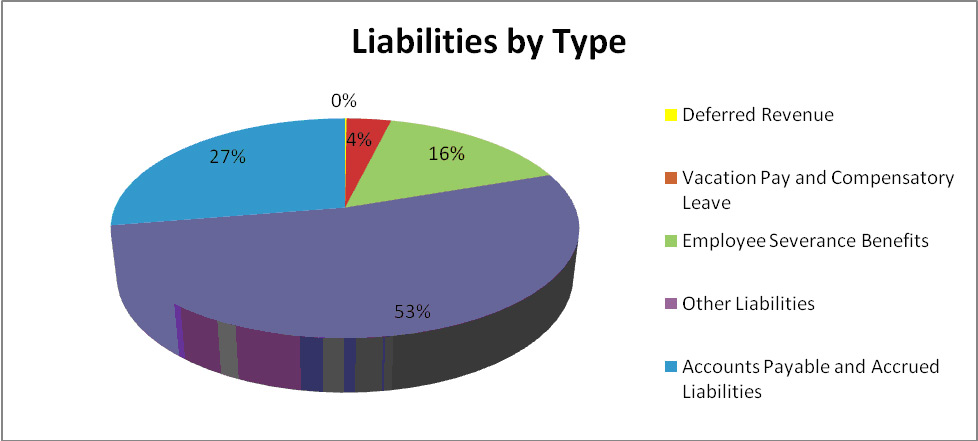
Total liabilities were $1,111.3M at the end of 2010-11, a decrease of $145.0M from the previous year. $92.5M of the net decrease in liability is a result of payments and interest earned and deemed to be payments against the Canada Health Infoway Inc. Liability from Budget 2009 and Budget 2007. Accounts payable and accrued liabilities decreased by $56.7M. This decrease was partially offset by an increase to employee severance benefits of $5.8M. There were also minor reductions to deferred revenue and the liability for vacation pay and compensatory leave.
Expenses by Strategic Outcome
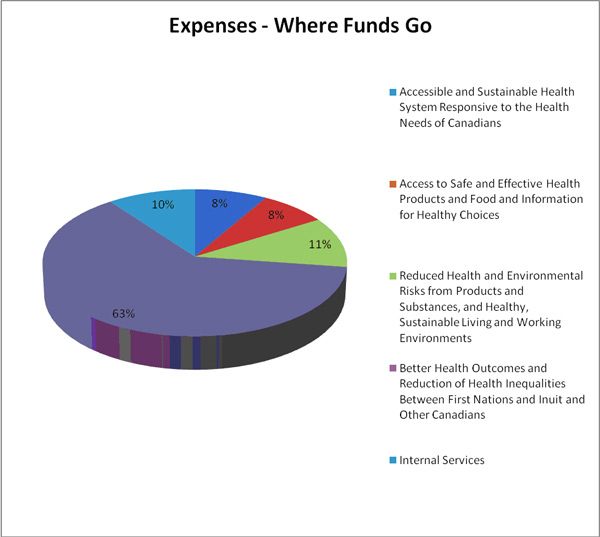
The department's total expenses were $3.8B in 2010-11, a decrease of $491.2M from 2009-10. This was due mainly to decreases in Transfer Payments ($521.9M) and Purchased Repair and Maintenance ($8.2M), offset by an increase in Professional and Special Services of $20.1M, Information $7.0M and Other $11.8M.
Revenues by Strategic Outcome
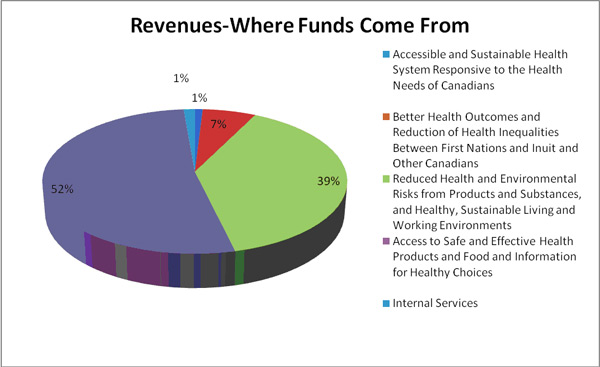
Health Canada receives most of its funding through annual Parliamentary appropriations. The Department uses the Consolidated Revenue Fund (CRF) which is administered by the Receiver General for Canada. All cash received is deposited to the CRF and all cash disbursements are paid from the CRF. Health Canada does however generate revenue from program activities that support the above-noted Strategic Outcomes. The Department's total revenue was $91.0M in 2010-11, an increase of $6.0M over 2009-10.
Financial Statements
Refer to the full Statement of Management Responsibility for further details:
2010-2011 Statement of Management Responsibility
List of Supplementary Information Tables
All electronic supplementary information tables found in the 2010-11 Departmental Performance Report can be found on the Treasury Board of Canada Secretariat's website.
- Sources of Respendable and Non-Respendable Revenue
- User Fees Reporting
- Status Report on Transformational Projects and Major Crown Projects
- Details on Transfer Payment Programs (TPPs)
- Up-Front Multi-Year Funding
- Horizontal Initiatives
- Green Procurement
- Response to Parliamentary Committees and External Audits
- Internal Audits and Evaluations
- G8/G20
Web Links
Aboriginal Diabetes Initiative
Aboriginal Head Start On Reserve
Aboriginal Health Human Resources Initiative
Aboriginal health programs in Budget 2010
Aboriginal Health Transition Fund
Air Quality Health Index (AQHI)
Alignment to Government of Canada Outcomes
Assisted Human Reproduction (AHR)
Assisted Human Reproduction Act
Biologics and Radiopharmaceuticals
Canada Consumer Product Safety Act
Canadian Adverse Reaction Newsletter
Canadian Agency for Drugs and Technologies in Health (CADTH)
Canadian Community Health Survey
Canadian Consumer Product Safety Act
Canadian Environmental Protection Act
Canadian Food Inspection Agency
Canadian Food Inspection Agency Act
Canadian Tobacco Use Monitoring Survey
Chemicals Management Action Plan
Controlled Drugs and Substances Act
Cracking Down on Tobacco Marketing Aimed at Youth Act
Drinking Water Advisory Module
Drug Safety and Effectiveness Network (DSEN)
Drug Treatment Funding Program
Enhancing labelling for food allergens, gluten sources and added sulphites
Evaluation of the Patient Wait Times Guarantees Pilot Project Fund
Federal Sustainable Development Act
Federal Tobacco Control Strategy
Food and Consumer Safety Action Plan
Health Human Resource Strategy
Health Service Integration Fund
Healthy Canadians: A federal report on comparable health indicators, 2008
Internationally Educated Health Professionals Initiative
Marihuana Medical Access Regulations
11th Ministerial Meeting of the Global Health Security Initiative
National Aboriginal Youth Suicide Prevention Strategy
National Pesticides Compliance Program
Negotiations in British Columbia
Negotiations with the Administration for Quality Supervision Inspection and Quarantine
Nutrition Facts Education Campaign
Official Language Minority Communities
Organization for Economic Co-operation and Development
Pan American Health Organization (PAHO)
Pest Management Regulatory Agency
Public Health Agency of Canada
Radiation Emitting Devices Act
Safe Drinking Water for First Nations Act
Sodium Reduction Strategy for Canada
Statistics Canada. Cansim Table 105-0501
The Internationally Educated Health Professionals Initiative
The 11th Ministerial Meeting of the Global Health Security Initiative
Unprocessed Product Licence Application Regulations