
Treasury Board of Canada Secretariat
www.tbs-sct.gc.ca
Common menu bar links
Breadcrumb Trail
ARCHIVED - Health Canada
 This page has been archived.
This page has been archived.
Archived Content
Information identified as archived on the Web is for reference, research or recordkeeping purposes. It has not been altered or updated after the date of archiving. Web pages that are archived on the Web are not subject to the Government of Canada Web Standards. As per the Communications Policy of the Government of Canada, you can request alternate formats on the "Contact Us" page.
Section 1 - 2008-2009 Departmental Overview
Minister's Message

This Departmental Performance Report is a synopsis of the work done by Health Canada in 2008-2009 to turn Government policy into tangible results for all Canadians.
In the last year, the Department has made important changes to help better protect and promote the health of Canadians. We have introduced new legislation to modernize and strengthen product safety laws -- legislation that will strengthen the Government's ability to respond when unsafe products are identified on the Canadian market. We have also taken additional steps to improve the safety and effectiveness of drugs on the market and to identify chemicals that may be harmful to Canadians. In 2008, we became the first country in the world to take steps towards a ban of Bisphenol A, a chemical that poses risks to infants and young children.
Through a range of programs, we have worked with communities in provinces and territories to help prevent and address addiction to drugs, alcohol and tobacco – especially among the young.
First Nations and Inuit health is an ongoing Health Canada responsibility and, in the last year, the Department made clear progress in enhancing community health programs for maternal and child health, mental health and suicide prevention. In partnership with other government departments, Health Canada supported communities as they took action to improve the quality of their drinking water and to address drug and alcohol addiction and communicable diseases. The Department bolstered many essential ongoing health services, such as those provided by nursing and other staff at facilities in First Nations and Inuit communities all over Canada.
Together with provinces and territories we made progress on common goals such as patient wait times and the transition to electronic health records. Collectively we also made progress on challenges such as the shortage of trained personnel in health care, exploring innovative approaches to providing services and seeking to facilitate the accreditation of internationally-trained professionals.
It was also a year during which we laid the groundwork for important advances in scientific research. In collaboration with The Canadian Institutes of Health Research (CIHR), we established a research consortium to advance cancer stem cell research. Funding was also provided for important research into obesity, diabetes, cardiovascular disease and into how to improve the health of children suffering from asthma and allergies.
We also worked hard with the Canadian Food Inspection Agency and the Public Health Agency of Canada to examine the factors that contributed to the August 2008 listeriosis outbreak and implement measures to help prevent and address a similar occurrence in the future.
Good health is important to every Canadian and the Government of Canada is proud to be a partner in enabling Canadians to achieve the best health outcomes possible. This Departmental Performance Report describes how Health Canada took action in 2008-2009 to deliver on the Government's commitment to safeguard the health of all Canadians.
The Honourable Leona Aglukkaq, P.C. M.P.
Minister of Health
Raison d'�tre
Health Canada is responsible for helping Canadians maintain and improve their health. It is committed to improving the lives of all Canadians and to making this country's population among the healthiest in the world as measured by longevity, lifestyle and effective use of the public health care system.
Responsibilities
Health Canada helps Canadians maintain and improve their health through various roles and responsibilities. First, as a regulator, the Department is responsible for the regulatory regime governing the safety of a broad range of products affecting the lives of all Canadians, including food, pharmaceuticals, medical devices, natural health products, consumer products, chemicals, radiation emitting devices, cosmetics, and pesticides. Health Canada also regulates tobacco products and controlled substances, public health on passenger conveyances, and helps manage the risks posed by environmental factors such as air, water, radiation in the workplace and environmental contaminants. This responsibility also extends to using cutting-edge science to assess and mitigate health risks to Canadians.
The Department is also a service provider. The federal government has provided basic health services to First Nations since 1904. Today, Health Canada supports the delivery of basic primary care services in approximately 200 remote First Nations communities, home and community care in more than 600 First Nations and Inuit communities, and a limited range of medically necessary health-related goods and services not insured by private or other public health insurance plans to eligible First Nations and Inuit. The Department also funds or delivers community-based programs and public health activities that promote health, prevent chronic disease and control the spread of infectious diseases. Health Canada directly employs approximately 650 nurses, operates 225 health centres and 61 alcohol and drug treatment centers, and supports more than 6,800 community-based workers employed by First Nations communities.
Finally, in the context of health systems, Health Canada is a catalyst for innovation, a funder, and an information provider. It works closely with provincial and territorial governments to develop national approaches on health system issues and promotes the pan-Canadian adoption of best practices. The Department administers the Canada Health Act, which embodies national principles to ensure a universal and equitable publicly-funded health care system. It provides policy support for the federal government's Canada Health Transfer to provinces and territories, and provides funding through grants and contributions to various organizations to help meet Health Canada's objectives. Lastly, it generates and shares knowledge and information on which personal decision-making, regulations and standards, and innovation in health rely.
Health Canada's Strategic Outcomes and Program Activity Architecture 2008 - 2009
The chart below illustrates Health Canada's framework of program activities and sub-activities contributing to progress toward the Department's strategic outcomes:
-
Strategic Outcome 1 - Accessible and Sustainable Health System Responsive to the Health Needs of Canadians
- Program Activity 1.1: Canadian Health System
- Key Program Sub-Activities:
- Canada Health Act Administration
- Official Language Minority Community Development
- Health System Renewal
- Health Information
- Women's Health
- Key Program Sub-Activities:
- Program Activity 1.2: Assisted Human Reproduction
- Program Activity 1.3: International Affairs
- Program Activity 1.1: Canadian Health System
-
Strategic Outcome 2 - Access to Safe and Effective Health Products and Food and Information for Healthy Choices
- Program Activity 2.1: Health Products
- Key Program Sub-Activities:
- Pharmaceutical Human Drugs
- Biologics and Radiopharmaceuticals
- Medical Devices
- Veterinary Drugs
- Natural Health Products
- Key Program Sub-Activities:
- Program Activity 2.2: Food and Nutrition
- Key Program Sub-Activities:
- Food Borne Pathogens
- Food Borne Chemical Contaminants
- Novel Foods
- Nutrition
- Key Program Sub-Activities:
- Program Activity 2.1: Health Products
-
Strategic Outcome 3 - Reduced Health and Environmental Risks from Products and Substances, and Healthy, Sustainable Living and Working Environments
- Program Activity 3.1: Sustainable Environmental Health
- Key Program Sub-Activities:
- Climate Change
- Air Quality
- Water Quality
- Chemicals Management
- Contaminated Sites
- Environmental Radiation Protection
- Passenger Conveyances
- Emergency Preparedness
- Key Program Sub-Activities:
- Program Activity 3.2: Consumer Products
- Key Program Sub-Activities:
- Consumer Product Safety
- Cosmetics
- Radiation Emitting Devices
- Key Program Sub-Activities:
- Program Activity 3.3: Workplace Health
- Key Program Sub-Activities:
- Public Service Health
- Internationally Protected Persons Health
- Workplace Hazardous Materials Information System
- Employee Assistance Services
- Dosimetry Services
- Key Program Sub-Activities:
- Program Activity 3.4: Substance Use and Abuse
- Key Program Sub-Activities:
- Tobacco
- Alcohol
- Controlled Substances
- Key Program Sub-Activities:
- Program Activity 3.5: Pesticide Regulation
- Key Program Sub-Activities:
- Evaluation of New Products
- Re-evaluation of Older Products
- Compliance and Enforcement
- Pesticide Risk Reduction
- Key Program Sub-Activities:
- Program Activity 3.1: Sustainable Environmental Health
-
Strategic Outcome 4 - Better Health Outcomes and Reduction of Health Inequalities between First Nations and Inuit and Other Canadians
- Program Activity 4.1: First Nations and Inuit Health Programming and Services
- Key Program Sub-Activities:
- First Nations and Inuit Community Programs
- First Nations and Inuit Health Protection and Public Health
- First Nations and Inuit Primary Care
- Non-Insured Benefits (supplementary) for First Nations and Inuit
- Governance and Infrastructure Support to First Nations and Inuit Health System
- Key Program Sub-Activities:
- Program Activity 4.1: First Nations and Inuit Health Programming and Services
Performance Summary: Financial and Human Resources Table
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 3,195.3 | 3,690.0 | 3,668.1 |
| Planned | Actual | Difference |
|---|---|---|
| 9,106 | 9,158 | 52 |
Performance Summary1
Health Canada applied the performance status rating as defined by Treasury Board of Canada Secretariat in their Guide to the Preparation of Part III of the 2009-10 Estimates.
- Exceeded --
- More than 100 per cent of the expected level of performance (as evidenced by the indicator and target or planned activities and outputs) for the expected result or priority identified in the corresponding RPP were achieved during the fiscal year.
- Met All --
- 100 per cent of the expected level of performance (as evidenced by the indicator and target or planned activities and expected outputs) for the expected result or priority identified in the corresponding RPP was achieved during the fiscal year.
- Mostly Met --
- 80 to 99 per cent of the expected level of performance (as evidenced by the indicator and target or, in the absence of targets, planned activities and expected outputs) for the expected result or priority identified in the corresponding RPP were achieved during the fiscal year.
- Somewhat Met --
- 60 to 79 per cent of the expected level of performance (as evidenced by the indicator and target or planned activities and outputs) for the expected result or priority identified in the corresponding RPP were achieved during the fiscal year.
- Not Met --
- Less than 60 per cent of the expected level of performance (as evidenced by the indicator and target or planned activities and outputs) for the expected result or priority identified in the corresponding RPP were achieved during the fiscal year.
1 The Health Canada 2008-2009 Report on Plans and Priorities (RPP) included an extensive range of performance indicators. Most did not have specifically defined targets. As such, the most appropriate synopsis for the year is provided by linking the expected results set out in the RPP with information on targets and results where available as well as other relevant performance evidence.
Departmental Priorities
The 2008-2009 Report on Plans and Priorities identified the following priorities for Health Canada
- Priority 1 - Contribute to the improvement of the health of Canadians (ongoing)
- Priority 2 - Reduce the risks to the health of the people of Canada (ongoing)
- Priority 3 - Work with others to strengthen the efficiency and effectiveness of the publicly-funded health care and health system (ongoing)
- Priority 4 - Strengthen accountability to Parliament and the public (ongoing)
These broad medium-term priorities, their strategies, and actions are addressed effectively in Health Canada's Management Priorities, which are described below under each strategic outcome, followed by the Health Canada Operational Priorities.
Management Priorities
Strategic Outcome 1: Accessible and sustainable health system responsive to the health needs of Canadians
Health Canada continued to implement Government of Canada commitments to work with provinces, territories and stakeholders for health system improvement. High-profile efforts with clear benefits for individual Canadians centred on initiatives testing approaches to reduce patient wait times and expand numbers of health professionals and other trained staff in place to provide services.
This strategic outcome links to Departmental Priorities 1, 3 and 4.
| Expected Results | 2008-09 Performance (Ongoing) Status: Mostly met |
|---|---|
| Canadian Health System: | |
| Improved health care system planning and performance | Implementation and monitoring of Government of Canada health commitments took place, including 12 Patient Wait Times Guarantees Pilot Projects implemented in eight jurisdictions. |
| Enhanced capacity of governments and stakeholders to support health system planning | Progress on the Pan-Canadian Health Human Resources (HHR) Strategy, included support for integration of internationally educated health professionals into the Canadian health care system and innovative ways to address HHR needs. |
| Awareness and understanding among health sector decision-makers and the public of the factors affecting accessibility, quality and sustainability of Canada's health-care system and the health of Canadians | Accountability to Canadians and Parliament was enhanced through the annual Healthy Canadians - A Federal Report on Comparable Health Indicators 2008, with an increase from 18 to 37 reported health indicators. |
| Canadian Assisted Human Reproduction (AHR): | |
| Collection of relevant and timely information in AHR practices including the number of stakeholders in AHR sector and details of their activities | Publishing of draft regulations deferred until after the Supreme Court of Canada releases its opinion on constitutional issues related to the AHR Act. |
| Number of proposed regulations related to AHR activities using own gametes published in Canada Gazette, Part I | |
| Reports of relevant issues addressed through a number of regulations and other instruments developed to enforce the AHR Act | |
| International Health Affairs: | |
| Enhanced knowledge base and intersectoral collaboration on global health issues | Active engagement in health initiatives on the international stage with other countries and through multilateral organizations (WHO, PAHO, OECD, APEC) helped to address issues such as regulatory cooperation, pandemic influenza preparedness, HIV/AIDS and global health security, and to influence global health policies, standards and actions. |
| Influencing the global health agenda for the benefit of Canadians | |
| Developed global health policies for the benefit of Canadians | |
| Program Activity | 2007-08 Actual Spending |
2008-09 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | |||
| Canadian Health System | 1,342.5 | 306.2 | 306.3 | 538.5 | 533.9 | Healthy Canadians |
| Canadian Assisted Human Reproduction | 5.7 | 2.0 | 2.1 | 3.9 | 3.9 | |
| International Health Affairs | 8.9 | 28.6 | 28.7 | 26.1 | 25.6 | |
| Total | 1,357.1 | 336.8 | 337.1 | 568.5 | 563.4 | |
Strategic Outcome 2: Access to safe and effective health products and food and information for healthy choices
Health Canada continued to improve its administration of regulatory processes for health and food products in Canada as part of the Food and Consumer Safety Action Plan, resulting in more timely reviews of new products. Resources were reallocated to address confirmed or possible threats to health to better respond to the interests of Canadians and the information available to Canadians on food and health products was expanded.
This strategic outcome links to Departmental Priorities 1, 2 and 4.
| Expected Results | 2008-09 Performance (Ongoing) Status: Mostly met |
|---|---|
| Health Products: | |
| Increased regulatory system response to health product-related health risks | Under the Food and Consumer Safety Action Plan, continued progress was demonstrated in timeliness of reviews, particularly for new drug submissions, as well as through fewer recalls of human drugs, veterinary drugs and natural health products, and Departmental responses to reported health product incidents improved over 2007-2008 levels. |
| Increased awareness and/or knowledge of health products issues | Expanded outreach to consumers, industry, and health professionals was matched by substantial evidence of public, professional and stakeholder interest in Health Canada reporting on and response to issues with health products identified by industry, health professionals and government, such as reports of adverse drug reactions. |
| Food and Nutrition: | |
| Reduction in exposure to disease-causing food-borne micro-organisms and environmental agrochemical contaminants, and food allergens | New resources enabled Health Canada to act on commitments in areas such as proposed new food labelling requirements, a risk management strategy to limit the exposure of newborns and young children to Bisphenol A and continued declines in transfat levels in food. They also enabled a rapid response to emerging issues of high priority to Canadians including support to the Canadian Food Inspection Agency during its major listeriosis investigation. |
| Increased level of informed choices/ healthy decisions related to food quality and food safety | Wide-ranging communications initiatives were implemented through printed documents such as the Canada's Food Guide in English and French and eight other languages, campaigns addressed particular food safety issues such as proper food handling procedures, information was also conveyed through extensive use of the Internet, contact with news media and presentations to audiences. |
| Program Activity | 2007-08 Actual Spending |
2008-09 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | |||
| Health Products | 207.1 | 183.3 | 186.5 | 257.1 | 255.9 | Healthy Canadians |
| Food and Nutrition | 100.8 | 77.6 | 77.9 | 65.0 | 61.7 | |
| Total | 307.9 | 260.9 | 264.4 | 322.1 | 317.6 | |
Strategic Outcome 3: Reduced health and environmental risks from products and substances, and healthy, sustainable living and working environments
New resources and improved processes enabled improved action on consumer and other product safety issues as well as departmental monitoring of substances that may have health impacts on Canadians under the Food and Consumer Safety Action Plan, the Clean Air Agenda and the Chemicals Management Plan. This was complemented by continued progress in reducing tobacco use and in supporting action against illicit drug use in Canada's communities.
This strategic outcome links to Departmental Priorities 1, 2 and 4.
| Expected Results | 2008-09 Performance (Ongoing) Status: Mostly met |
|---|---|
| Sustainable Environmental Health: | |
| Timely regulatory system response to new and emerging health risks related to toxic chemicals and environmental risks to health | Health Canada service commitments such as reviews of potentially toxic chemicals, inspections of passenger conveyances, emergency preparedness exercises and risk assessments of contaminated sites were fully met. |
| New and emerging health risks related to toxic chemical substances are identified, assessed and managed | Under the Chemicals Management Plan (CMP), 9 of 12 batches of substances with possible health or environment concerns were either under review or fully reviewed, meeting all CMP Challenge timelines. |
| Canadians are knowledgeable and aware of environmental health issues | The Air Quality Health Index (AQHI) was made available in 26 locations across Canada, including 10 census metropolitan areas (target is approximately 27 census metro areas by 2011), while 23% of Canadians reported hearing about federal activities on chemicals and 7% were aware of the Chemicals Management Plan. |
| Consumer Products: | |
| Declining trends in levels of risk, adverse reactions, illnesses, and injuries from hazardous products, substances, cosmetic products, and radiation emitting devices | Improved effectiveness in recording and responding to complaints was achieved via more inspectors in the regions receiving and responding to complaints, better tracking, and new service standards for complaint response. |
| Adherence to Acts and Regulations | Targeted surveillance activities lead to the early identification of emerging risks, rapid response and enforcement actions. Inspection cycles showed no significant changes in levels of industry compliance in two broad product categories and saw consistently high levels of compliance in other product categories. Where non-compliance was found, product recalls, seizures and advisories were used to address the issue. |
| Canadians are knowledgeable/aware of the health risks of exposure to hazardous products, substances, cosmetic products, and radiation emitting devices | Increased Canadian awareness was indicated by 2,400 more subscriptions to the Consumer Product Safety Recall website, raising the total to 6,600. |
| Workplace Health: | |
| Timely system response to public service employees with psycho-social problems | 93% of public service employee clients' psycho-social problems were addressed within service standards (target: 70%). |
| Internationally Protected Persons (IPPs) and Canadian public service employees are protected during visits and events from work-related and other risks to their health and safety | No serious health related incidents occurred involving IPPs and surveys found 100% of clients were satisfied (target: 80%). |
| Adherence to Acts, Regulations, and Guidelines | A review was identified for Health Canada Workplace Hazardous Material Information System responsibilities to address weaknesses. |
| Substance Use and Abuse: | |
| Smoking prevalence rate | The Canadian smoking prevalence rate (the proportion of Canadians who smoke) declined from 21.7% in 2001 to 17.9% in the first half of 2008. |
| Reduced tobacco consumption | Cigarette consumption in Canadian smokers declined from 17 cigarettes smoked per day in 1999 to 15 per day in 2008. |
| Reduced abuse of drugs, alcohol, and other controlled substances | While no measures are yet in place for prevalence rates, actions were taken through the National Anti-Drug Strategy to support community responses and provide support for law enforcement. The Department's planned progress on alcohol consumption initiatives was delayed. |
| Pesticide Regulation: | |
| Declining trends in levels of risk from regulated pest control products | Development continued of the baseline data needed to measure declining trends in risk levels from regulated pest control products and a first annual report was produced. |
| Increased stakeholder awareness of risks and confidence in regulatory activities | A survey provided baseline data to measure stakeholder satisfaction with Canada's pesticide regulatory system that will enable future progress to be tracked. |
| Program Activity | 2007-08 Actual Spending |
2008-09 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | |||
| Sustainable Environmental Health | 126.4 | 166.1 | 165.4 | 172.9 | 165.5 | Healthy Canadians |
| Consumer Products | 25.9 | 24.1 | 24.2 | 29.4 | 29.4 | |
| Workplace Health | 56.8 | 34.2 | 34.8 | 51.5 | 51.5 | |
| Substance Use and Abuse | 125.4 | 152.7 | 152.9 | 118.5 | 118.4 | |
| Pesticide Regulation | 58.9 | 60.3 | 60.5 | 66.4 | 64.5 | |
| Total | 393.4 | 437.4 | 437.8 | 438.7 | 429.3 | |
Strategic Outcome 4: Better health outcomes and reduction of health inequalities between First Nations and Inuit and other Canadians
With new resources from Budget 2008, Health Canada was able to continue to help address the health issues facing First Nations and Inuit. Supported by investments in innovative approaches to health service delivery and the negotiation of tripartite agreements, the Department continued to work with willing partners to improve health service delivery through the increased integration and harmonization of federal and provincial/territorial health systems. In addition to maintaining essential health programs and services, Health Canada helped to expand improved drinking water supply monitoring and helped to address priority issues such as youth suicide and mental wellness through the establishment of a mental wellness team, mental health promotion demonstration projects and community-based suicide prevention projects.
This strategic outcome links to Departmental Priorities 1, 2, 3 and 4.
| Expected Results | 2008-09 Performance2 (Ongoing) Status: Mostly met |
|---|---|
| Strengthened community programs; better health protection; improved primary health care; and access to Non-Insured Health Benefits (NIHB) to contribute to improved health status of First Nations and Inuit individuals, families and communities | Sustainable Environmental Health: |
| Life Expectancy - The most recent data (2001) estimated life expectancy for First Nations at 70.4 years for males and 75.5 years for females; and for Inuit at 64.4 years for males and 69.8 years for females (Canadian averages: males 77 years, females 82 years). | |
| Birth weight - The most recent data (2000) indicated that 4.7% of First Nations births were classified as low birth weight (5.6% Canadian average) and 21% were high birth weight (13% Canadian average). | |
| The most recent Non-Insured Health Benefits program utilization rate (2007-2008) was 64% (the percentage of clients who received at least one pharmacy benefit paid as a proportion of the total number of eligible clients). | |
| Sustainable Environmental Health: | |
| The Department took action on community program priorities (e.g., Patient Wait Times Guarantees Pilots, Maternal and Child Health Program, Aboriginal Head Start On Reserve, National Aboriginal Youth Suicide Prevention Strategy, Action Plan for First Nations and Inuit Mental Wellness). | |
| Health Canada took action on public health priorities (e.g., drinking water quality improvement support, communicable disease prevention and control programs, improved environmental health risk management). | |
| Departmental support for primary health care programs included substantial attention to recruiting and retaining professional and other health human resources needed to provide these and other programs and services. | |
| Actions took place on a range of governance and infrastructure priorities (e.g., quality improvement activities, community capacity building, improved access to funds for First Nations, Inuit, and M�tis students pursuing health career studies, investments and agreements to support increased integration and harmonization of federal and provincial / territorial health systems, and investments in on-reserve health facilities and staff residences). |
| Program Activity | 2007-08 Actual Spending |
2008-09 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | |||
| First Nations and Inuit Health Programming and Services | 2,227.6 | 2,155.6 | 2,156.0 | 2,360.7 | 2,357.8 | Healthy Canadians |
| Total | 2,227.6 | 2,155.6 | 2,156.0 | 2,360.7 | 2,357.8 | |
2 The performance summary for this strategic outcome reflects high-level performance indicators for First Nations and Inuit health outcomes as well as descriptions of key Health Canada initiatives.
Operational Priorities
In addition to performance linked to departmental priorities and the strategic outcomes, Health Canada is in the process of transforming internal services to support more efficient program delivery by the Department and its Health Portfolio partners.
Human resources (HR) practices were realigned to meet the needs of both present and future workforces. This business investment saw the establishment of Enterprise HR and implementation of innovative methods for service delivery with concentration in science and technology staffing. These transformation activities have positioned the Department to be the workplace of choice among federal science-based departments.
In similar fashion, the development of a long-term laboratory strategy and a Real Property Management Framework identified necessary laboratory refurbishments and began the foundation for a long-term office accommodation plan. The outcomes have resulted in many benefits, including lower operating costs where possible.
The Department's participation in the government-wide Shared Services Initiative has yielded a comprehensive benchmarking study on a distributed computing environment, major consolidation, and new efficiencies in Information Technology (IT) service delivery. While the Enterprise IT project continued to progress, it encountered resource challenges, moving some implementation into 2009-2010. The information management agenda advanced through implementation of a Proof of Concept project and the subsequent rollout of an electronic document management system in a limited number of Health Canada branches.
Management Improvement Initiatives
Human resources planning was more fully integrated into the departmental business planning process. The broader objective was to reach full integration of planning activities for all functional areas into one coherent planning process. As a result, the 2009-2010 Departmental Operational Plan outlines the full breadth of planned departmental activities for the fiscal year, together with their expected results and performance targets. It also integrates planned activities with information about requirements for human resources, information management, information technology, finance, procurement and facilities. Integration has improved the efficiency and effectiveness of planning activities.
Consistent and standardized departmental processes were implemented in the area of financial management, including the development of the Budget Management Framework. An independent Departmental Audit Committee was also fully implemented, providing additional departmental oversight. To support the efforts to have the Department ready for the audit of its financial statements in 2011, an action plan was presented to the Office of the Comptroller General on a quarterly basis. In addition, the Department explored and then agreed to provide certain financial management services to the Canada School of Public Service, as of 2009-2010.
An Integrated Risk Management Framework for Grants and Contributions was approved in 2008 with an Enterprise Risk Management software application being developed to harmonize risk management practices for transfer payments across the Health Portfolio. The Department also continued to apply the Management Accountability Framework (MAF) and integrate MAF expectations into the management culture.
Risk Analysis
As indicated in the Report on Plans and Priorities for 2008-2009, Health Canada manages a diverse range of risks in the course of ongoing planning and management. During the year, the Department took action in several health-related areas as either lead or partner in coordinated efforts with other government and non-government organizations to address incidents of actual or potential impact on the health of Canadians.
During the food-borne listeriosis contamination situation during the summer of 2008, Health Canada worked with partners to minimize the impact of the outbreak on Canadians, as described elsewhere in this report. While the Department addressed the outbreak proactively, this incident highlighted the large number of external partners with whom activities need to be coordinated and importance of having clear roles and responsibilities to respond effectively to challenges and to manage risks during that work.
As part of work under the Chemicals Management Plan, Canada became the first country to address the risks associated with Bisphenol A (BPA), a widely-used chemical compound found in some hard, clear, lightweight plastics and resins. Health Canada had to weigh research findings against the health risk to a particularly vulnerable segment of the population, infants up to the age of 18 months, which led to a Government decision to move forward with regulations to prohibit the importation, sale and advertising of polycarbonate baby bottles that contain Bisphenol A.
Health Canada's programs and services for First Nations and Inuit are essential to helping to obtain better health outcomes and reduce the health inequalities between First Nations and Inuit and other Canadians. Health Canada has managed the risk associated with maintaining these programs and services in order to ensure adequate disease prevention and control in the face of cost pressures created by factors including rapidly-growing First Nation and Inuit populations and increased health care costs for a number of years. Budget 2008 helped to respond to this risk by providing funding to stabilize essential health services in 2008-09, support health system innovations and support the negotiation of Tripartite Agreements with willing provinces and First Nations. These investments will help strengthen the current health programs that help to improve First Nations and Inuit health outcomes, as well as support the system to become more efficient and effective through greater integration and harmonization with provincial/territorial health systems.
Expenditure Profile
For the 2008-09 fiscal year, Health Canada spent $3,668.1 million to meet the expected results of its program activities and contribute to its strategic outcomes.
In 2008, Health Canada conducted a Strategic Review of the funding, relevance and performance of all its programs and spending to ensure results and value for money from programs that are a priority for Canadians. The results of this Review will be reflected in future reporting to Parliament.
The figure below illustrates Health Canada's spending trend from 2006-07 to 2008-2009.
Spending Trend
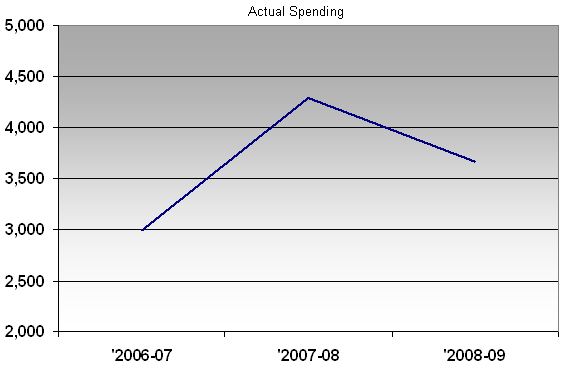
For the 2006-07 to 2008-09 periods, the total spending includes all Parliamentary appropriation sources: Main Estimates, Supplementary Estimates, Treasury Board collective bargaining, operating budget carry forward, and other special adjustments.
In 2007-08, actual spending was particularly high due to the $1B compensation payments to individuals infected with the Hepatitis C virus through the Canadian blood supply before 1986 and after 1990.
The table below offers a comparison of the Main Estimates, planned spending, total authorities and actual spending for the most recently completed fiscal year, as well as the historical actual spending figures for the previous year.
| Program Activity | 2007-08 Actual Spending |
2008-09 | |||
|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | ||
| Canadian Health System | 1,342.5 | 306.2 | 306.3 | 538.5 | 533.9 |
| Canadian Assisted Human Reproduction | 5.7 | 2.0 | 2.1 | 3.9 | 3.9 |
| International Health Affairs | 8.9 | 28.6 | 28.7 | 26.1 | 25.6 |
| Health Products | 207.1 | 183.3 | 186.5 | 257.1 | 255.9 |
| Food and Nutrition | 100.8 | 77.6 | 77.9 | 65.0 | 61.7 |
| Sustainable Environmental Health | 126.4 | 166.1 | 165.4 | 172.9 | 165.5 |
| Consumer Products | 25.9 | 24.1 | 24.2 | 29.4 | 29.4 |
| Workplace Health | 56.8 | 34.2 | 34.8 | 51.5 | 51.5 |
| Substance Use and Abuse | 125.4 | 152.7 | 152.9 | 118.5 | 118.4 |
| Pesticide Regulation | 58.9 | 60.3 | 60.5 | 66.4 | 64.5 |
| First Nations and Inuit Health Programming and Services | 2,227.6 | 2,155.6 | 2,156.0 | 2,360.7 | 2,357.8 |
| Total Department | 4,286.0 | 3,190.7 | 3,195.3 | 3,690.0 | 3,668.1 |
The $4.6 million increase from Main Estimates to planned spending is due to anticipated funding for the renewal of the Genomics Research and Development Initiative and for public health and health-related responsibilities relating to the 2010 Olympic and Paralympic Winter Games.
The $494.7 million increase from planned spending to total authorities was due to new funding received through Supplementary Estimates, including funding for accelerating First Nations and Inuit Health's tripartite negotiations in British Columbia and investments in health innovation and core health services for First Nations, implementing First Nations Water and Wastewater Action Plan, and strengthening and modernizing Canada's safety system for food, consumer and health products.
The $21.9 million difference between total authorities and actual spending was mainly the result of lapses in the Health Council special purpose allotment, the Indian Residential Schools special purpose allotment, and TB frozen allotments for the National Anti-Drug Strategy (Mandatory Minimum Penalties), the Access to Medicines Program, and the Capital Carry Forward.
Voted and Statutory Items
This table illustrates the way in which Parliament approved Health Canada's resources, and shows the changes in resources derived from Supplementary Estimates and other authorities, as well as how the funds were spent.
| Vote | 2007-08 Actual Spending |
2008-09 | |||
|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | ||
| Health Canada | |||||
| (1) Operating Expenditures | 1,823.3 | 1,661.6 | 1,666.2 | 1,894.7 | 1,884.7 |
| (5) Capital Expenditures | 0.0 | 60.0 | 60.0 | 48.0 | 40.9 |
| (10) Grants and Contributions | 1,258.0 | 1,358.1 | 1,358.1 | 1,393.8 | 1,389.6 |
| (S) Minister's Car Allowance & Salary | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 |
| (S) Spending of proceeds from the disposal of surplus Crown assets | 0.1 | 0.0 | 0.0 | 0.7 | 0.1 |
| (S) Refunds from Previous Years Revenue | 0.3 | 0.0 | 0.0 | 0.2 | 0.2 |
| (S) Hepatitis C virus through the Canadian blood supply before 1986 and after 1990 | 1,023.5 | 0.0 | 0.0 | 0.0 | 0.0 |
| (S) Canada Health Infoway Inc. | 38.7 | 0.0 | 0.0 | 123.0 | 123.0 |
| (S) Implementation Act | 30.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| (S) Transfer payments to Mental Health Commission of Canada | 0.0 | 0.0 | 0.0 | 110.0 | 110.0 |
| (S) Contributions to employee benefit plans | 112.0 | 110.9 | 110.9 | 119.5 | 119.5 |
| Total Department | 4,286.0 | 3,190.7 | 3,195.3 | 3,690.0 | 3,668.1 |
(S) Indicates expenditures the Department is required to make that do not require an appropriation act