
Common menu bar links
Breadcrumb Trail
ARCHIVED - Public Health Agency of Canada - Report
 This page has been archived.
This page has been archived.
Archived Content
Information identified as archived on the Web is for reference, research or recordkeeping purposes. It has not been altered or updated after the date of archiving. Web pages that are archived on the Web are not subject to the Government of Canada Web Standards. As per the Communications Policy of the Government of Canada, you can request alternate formats on the "Contact Us" page.
Minister's Message

I am pleased to present the Public Health Agency of Canada's 2012–13 Report on Plans and Priorities. Over the next three years, the Agency will advance a number of important initiatives in support of its mandate to promote and protect the health of Canadians. The Agency will continue to strengthen public health emergency preparedness and response capacity, provide national leadership in health promotion and health protection, and build public health capacity.
With increasing economic integration and the global movement of people and goods, public health issues know no borders. Public health is a shared responsibility and jurisdictions must work together to be effective in addressing public health challenges. The Agency will continue to work closely with domestic and international partners on collective efforts to deal with issues that impact the health of Canadians and to ensure that Canadians are equipped with the information and tools necessary to make informed decisions about their health and well-being.
In 2012–13, the Agency will focus on advancing the Political Declaration adopted at the September 2011 United Nations High-level Meeting on the Prevention and Control of Non-communicable Diseases, a declaration I was pleased to endorse. Our coordinated efforts will help to address the four major chronic diseases: cancer, diabetes, cardiovascular disease, and chronic respiratory disease, while also recognizing linkages to other diseases, including mental illness. Additionally, the Agency will continue its commitment to addressing childhood obesity through actions in support of Curbing Childhood Obesity: a Federal/Provincial/Territorial Framework for Action to Promote Healthy Weights.
Promoting the positive mental health and well-being of Canadians is an important step in reducing illness, disability, and injury, and helping Canadians live healthy lives. Issues associated with untreated mental health problems, including suicide, create a significant burden on individuals, families, and communities. The Agency will work to advance multi-sectoral collaboration and increase Canadians' awareness of these important public health issues.
In recent years, the Agency has made progress in its ability to prevent, detect and respond to food-borne illness outbreaks as part of Canada's food safety system. Food-borne illness outbreaks can present not only significant public health risks, but also have economic and trade implications for a country. The Agency will continue to strengthen its efforts in protecting Canadians from food-borne illness outbreaks.
The Public Health Agency of Canada is committed to ensuring that resources align with priorities so that the Agency can continue to deliver quality programs that meet the public health needs of Canadians.
I am confident in the Agency's ability to deliver on the priorities in this report and look forward to continued collaborative efforts to improve the health and well-being of Canadians.
Leona Aglukkaq, P.C., M.P.
Minister of Health
Message from the Chief Public Health Officer
In 2012–13, the Agency will build on its leadership role in protecting and promoting the health of Canadians through its stewardship, world-class science, research and surveillance, and effective collaboration with all our partners.
Chronic diseases such as cancer, diabetes, cardiovascular and respiratory diseases have a major impact, causing nearly 9 in 10 deaths each year in Canada. Building on national and international commitments in these areas, such as the landmark national Curbing Childhood Obesity: A Federal /Provincial/Territorial Framework for Action to Promote Healthy Weights, the Agency will continue efforts that help to promote health, prevent and mitigate disease, and reduce health inequalities. The Agency will continue to support best practices and initiatives, such as the Active and Safe Injury Prevention Initiative, which encourages children and youth to be active in recreational and sports activities while also promoting injury prevention. At the community level, the Agency's Innovation Strategy will also continue to support recognized interventions that help Canadians, particularly those at greater risk for poor health outcomes, improve their health.
As the world evolves, however, so do risks from our surrounding environment, such as the production, transport and use of human pathogens and toxins. The Agency will build on its novel approach to the development of new regulations and inspection, ensuring compliance with the new Human Pathogens and Toxins Act. It will also identify strategies to reduce regulatory red tape for industry, while ensuring that the environment and the health and safety of Canadians are not compromised.
In addition, an increasingly connected world means emerging and exotic infectious diseases pose significant threats to our health. Through global partnerships, the Agency will help sustain our preparedness for health emergencies, supported by a newly renewed pandemic vaccine supply. It will also enhance its communications about travel health, ensuring Canadians receive timely and accurate information for their safety.
Surveillance and research of many of these diseases and conditions form the backbone of the Agency's efforts. In 2012–13, the Agency will take a leadership role in building an autism surveillance system. Our surveillance and research activities will be supported by the maintenance of an already world-class, efficient and effective laboratory network across the country.
The Agency is taking the opportunity to adapt, lead, and innovate in its approach to public health in Canada. It will continue to increase its efficiency, streamline operations, and improve processes, supported by employees that make the Agency one of the world's best public health organizations. As an effective agent for positive change, the Agency is well-placed to serve Canadians and to meet the demands of the future. Please take the time to read this report, to learn more about how we are moving forward in protecting and promoting the public's health.
David Butler-Jones, M.D.
Chief Public Health Officer
Section I – Organizational Overview
Raison d'être
Public health involves the organized efforts of society to keep people healthy and to prevent injury, illness and premature death. It includes programs, services and policies that protect and promote the health of all Canadians. In Canada, public health is a responsibility that is shared by the three levels of government in collaboration with the private sector, non-governmental organizations, health professionals and the public.
In September 2004, the Public Health Agency of Canada (the Agency) was created within the federal Health Portfolio to deliver on the Government of Canada's commitment to increase its focus on public health in order to help protect and improve the health and safety of all Canadians and to contribute to strengthening the health care system.
Responsibilities
The Agency has the responsibility to:
- contribute to the prevention of disease and injury, and to the promotion of health;
- enhance the quality and quantity of surveillance data and expand the knowledge of disease and injury in Canada;
- provide federal leadership and accountability in managing public health emergencies;
- serve as a central point for sharing Canada's expertise with the rest of the world and for applying international research and development to Canada's public health programs; and
- strengthen intergovernmental collaboration on public health and facilitate national approaches to public health policy and planning.
Strategic Outcome and Program Activity Architecture (PAA)
The Agency aims to achieve a strategic outcome of the promotion of health, reduced health inequalities, and the prevention and mitigation of disease and injury, supported by its Program Activity Architecture depicted in the following figure.
[enlarge]
Organizational Priorities
| Priority | Type | Strategic Outcome or Program Activity |
|---|---|---|
| 1. Managing Public Health Risks to Canadians | Ongoing | PAA: 1.1, 1.2, 1.3, 1.5 and 1.6 |
| Why is this a priority? | ||
| Anticipating and proactively responding to real and potential health risks to Canadians will help prevent and mitigate disease and injury. | ||
| Plans for meeting the priority | ||
|
||
| 2. Promoting health and reducing health inequalities in Canada | Ongoing | PAA: 1.1, 1.2, 1.4 and 1.5 |
| Why is this a priority? | ||
| Improving health equity in Canada can realize significant benefit to overall public health through increased access to opportunities and conditions conducive to the health of all and the reduction of health inequalities. | ||
| Plans for meeting the priority | ||
|
||
| 3. Enhancing Public Health Capacity | Ongoing | PAA: 1.2, 1.3, 1.4, 1.5 and 1.6 |
| Why is this a priority? | ||
| Enhancing pan-Canadian and Agency capacity will contribute to building a stronger public health system and, in turn, promote health, reduce health inequalities and prevent and mitigate disease and injury. | ||
| Plans for meeting the priority | ||
|
||
| 4. Achieving Excellence in Governance and Management | Previously committed | PAA: 1.1, 1.6, and 2.1 |
| Why is this a priority? | ||
| Strengthening governance and management infrastructure will improve the Agency's ability to serve the public health interests and needs of Canadians. | ||
| Plans for meeting the priority: | ||
|
||
Risk Analysis
Public health involves the organized efforts of society to keep people healthy and to prevent injury, illness and premature death. In Canada, public health is a responsibility that is shared by the three levels of government in collaboration with the private sector, non-government organizations, health professionals and the public. The Public Health Agency of Canada (PHAC) plays a central role in chronic and infectious disease prevention and control, health promotion, injury prevention, and public health emergency management. PHAC carries out its responsibilities by providing leadership during, and building capacity for, public health emergencies, collaborating with public health partners, and facilitating approaches to public health policy and planning.
PHAC operates in an environment characterized by change, complexity, and uncertainty. For example, a long and sustained period of economic growth has been followed by periods of recession worldwide, and in some countries, financial crisis. With the global economy in a sluggish state, governments are making balanced budgets a priority. The resulting fiscal constraint influences individual and collective public health. This reinforces the value of the role, initiatives, and actions of PHAC and of its partners in promoting cost-effective healthy choices and healthy lifestyles.
Demographic factors also contribute to the challenge faced by PHAC and its partners. Among these, the following are worth noting.
- Canada's population is increasingly diverse, as it continues to be one of the world's major immigrant and refugee receiving countries. In twenty years, close to half of Canadians will be foreign born and one in three Canadians may also be members of a visible minority. Immigrants' experiences of post-migration health vary widely, obscuring important health disparities which exist among some subgroups.
- Canada's Aboriginal population is younger and growing nearly six times faster than the non-Aboriginal population. And while Aboriginal children represent an increasing proportion of Canada's children, they are disproportionately living in poverty and consistently experience poor health outcomes, including higher than average suicide rates.
- Canada's population is also aging; seniors are living longer and are healthier than in previous generations. With increasing age, however, the potential for individuals to suffer from multiple chronic conditions and dementia increases.
The above factors, and more, are testing the health system's capacity to respond effectively.
The impacts of chronic disease are significant, with the consequence of diminishing the quality of life for many Canadians and, in particular, for specific populations (e.g., Aboriginal and northern populations). Addressing chronic disease involves addressing social, economic and physical conditions that are complex and difficult to change. In addition, two health issues require attention as they are significant risk factors contributing to the development of chronic disease.
- Mental illness-related disability claims (short-term and long-term) account for up to one-third of workplace claims and approximately 70% of workplace costs—a $33-billion loss to the Canadian economy on an annual basis. People with serious mental illness are at higher risk of a wide range of chronic and physical conditions; the fastest growing of these are depression and anxiety disorders. By 2020, depression is projected to be the second-leading cause of disability in the world behind ischemic heart disease (i.e., local deficiency of blood supply).
- Increasing obesity rates contribute to an increased risk for chronic diseases such as diabetes, cardiovascular disease and hypertension. There are twice as many obese Canadian adults in Canada today than there were 25 years ago and currently, more than one in four children and youth in Canada are overweight or obese.
Similarly, sustained efforts are required to prevent and control new strains of infectious diseases which pose increasing and unpredictable threats to public health. For instance, inappropriate use of antimicrobials leads to pathogens becoming resistant to current treatments. Animal husbandry and wildlife management practices impact genetic changes in microorganisms giving rise to new pathogens. And the rapid global movement of people, animals and goods is facilitating global transport of new and existing infectious diseases.
Efforts to prepare for, and respond to, public health emergencies are undertaken in an environment where threats are also unpredictable and complex. Threats may be in the form of an infectious disease outbreak (such as Listeria in food) or pandemic (e.g., H1N1), natural events (such as floods and earthquakes), or intentional and unintentional man-made events involving chemical, biological, radiological, or nuclear hazards.
This reality is also true for the PHAC's partners, and more than ever, there is a need to work collaboratively and efficiently towards the achievement of shared objectives with a focus on disease and illness prevention initiatives. PHAC cooperates, coordinates, collaborates and partners with stakeholders such as other federal departments, provincial, territorial and local authorities, the World Health Organization, the United States Centers for Disease Prevention and Control, other international partners, and non-governmental organizations,. The need to advance objectives in concert with others impacts virtually all areas of the PHAC's work.
The Canadian public health work force is maturing and may see a loss of knowledge and experience as public health professionals retire. As a result, the importance of continued efforts to enhance the skills, knowledge and experience of public health professionals is growing.
PHAC's Corporate Risk Profile (CRP) identifies the most significant risks influencing priorities and outlines strategies to address them. Risk considerations are also factored into the planning of all PHAC programs, evaluations and audits and help to determine their priority and scope. The table below outlines the risks and opportunities identified in the 2011 CRP as well as the Program Activities where information on mitigation plans and strategies can be found.
| Risk Areas | Risk Statement | Program Activity |
|---|---|---|
| Infectious Disease | There is a risk that emerging infectious diseases will continue to create the potential for epidemics and pandemics that will result in considerable health, social and economic impacts. | 1.1, 1.2, 1.3, 1.5, 1.6 |
| There is a risk that antimicrobial resistance in disease-causing organisms will continue to be a threat to the Canadian population resulting in increased morbidity, mortality and impact on the health system. | 1.1, 1.2 | |
| Population Mobility and Migration | There is a risk that rising global population mobility—travel and migration—will increase infectious disease importation and chronic disease development, resulting in increased morbidity, mortality, and burden to the Canadian health system. | 1.2, 1.6 |
| Emergency Preparedness and Response | There is an opportunity for the Agency to enhance its emergency management capacity and to improve its ability to work with external partners to prepare for and provide leadership and coordination in the management of public health events on behalf of the federal government. | 1.2, 1.3, 1.5, 1.6 |
| Food-borne Illness | With current global trends in food production, preparation and distribution there is a continuing risk that food-borne illness will adversely impact the Canadian population with the potential for considerable health, social and economic consequences. | 1.1, 1.2, 1.5 |
| Aboriginal and Northern Health Inequalities | There is a risk that Aboriginal and northern populations will continue to experience poorer overall health outcomes, including higher rates of chronic and infectious diseases, than other Canadians. The persistent health inequalities are costly in human, social and economic terms, and are largely preventable. | 1.3, 1.4, 1.5 |
| Chronic Disease | There is a risk that obesity rates among Canadian adults, children and youth will continue to rise, increasing the rate of chronic diseases such as diabetes, cardiovascular disease and hypertension. | 1.2, 1.4, 1.5 |
| There is a risk that mental illness will continue to adversely impact the Canadian population resulting in significant health, social and economic costs. | 1.2, 1.4 | |
| Management Capability and Excellence | There is an opportunity for PHAC to enhance its management capacity in the areas of governance, planning, people management (e.g. values and ethics, training), finance, security, technology, etc. to support the Agency in fulfilling its public health mission and mandate. | 2.1 |
| Canadian Public Health Capacity | There is a risk that Canada lacks the appropriately trained work force, tools, organizational capability, and inter-jurisdictional systems to respond to and plan for public health threats. | 1.3, 2.1 |
Planning Summary
Financial Resources ($M)
| 2012–13 | 2013–14 | 2014–15 |
|---|---|---|
| 616.5 | 590.6 | 631.8 |
Note: Additional information on expenditures at the Agency level is provided in Section I's Expenditure Profile and at the Program Activity level in Section II.
Human Resources (Full-time Equivalent – FTE)
| 2012–13 | 2013–14 | 2014–15 |
|---|---|---|
| 2,668 | 2,667 | 2,675 |
Planning Summary Table
| Performance Indicators | Targets | ||||||
|---|---|---|---|---|---|---|---|
| An overall population health indicator for Canada is health-adjusted life expectancy* (HALE) at birth |
The Agency's objective is to work towards the maintenance or increase of Canada's 2001 HALE at birth as reported by Statistics Canada1
|
||||||
| An additional view of population health is HALE by income; i.e., the difference, in years, in HALE at birth between the top-third and bottom-third income groups |
The Agency's objective is to work towards the maintenance or reduction of the difference in years
|
*Health Adjusted Life Expectancy (HALE) is a composite, summary measure of population health. It is more comprehensive than the better-known Life Expectancy measure, as HALE combines length of life and health-related quality of life into a single indicator. HALE is defined as "the number of years in full health that an individual can expect to live given the current morbidity and mortality conditions."2
How long Canadians live in good health is determined by factors including personal and family lifestyle risk factors, environmental and genetic factors, technological advances, social determinants, availability and quality of health care, and public health practices and initiatives at the federal, provincial, territorial (F/P/T), and local levels of government. The Agency works with governmental and non-governmental stakeholders to positively affect the above factors of health. The results of these combined factors and efforts can best be assessed by looking at summary measures of population health.
PHAC contributes to maintaining or increasing HALE in Canada through all its programs. Undertaken in collaboration with F/P/T, non-governmental organizations and international health partners, these programs provide federal leadership and support in promoting health, reducing health disparities, enhancing public health capacity, preventing and mitigating injuries and chronic and infectious diseases, providing relevant research support, monitoring health and disease situations and trends, and reducing the risk and consequences of public health emergencies.
| Program Activity | Forecast Spending 2011–12 |
Planned Spending | Alignment to Government of Canada Outcomes | ||
|---|---|---|---|---|---|
| 2012–13 | 2013–14 | 2014–15 | |||
| 1.1 Science and Technology for Public Health | 69.1 | 65.4 | 59.4 | 58.0 | Healthy Canadians |
| 1.2 Surveillance and Population Health Assessment | 61.4 | 64.6 | 64.6 | 64.0 | |
| 1.3 Public Health Preparedness and Capacity | 120.0 | 85.1 | 71.3 | 67.0 | |
| 1.4 Health Promotion | 185.3 | 181.4 | 181.2 | 181.3 | |
| 1.5 Disease and Injury Prevention and Mitigation | 111.5 | 100.5 | 94.8 | 142.2 | |
| 1.6 Regulatory Enforcement and Emergency Response | 27.4 | 24.0 | 24.0 | 24.1 | Safe and Secure Canada |
| Total Planned Spending | 574.7 | 521.0 | 495.3 | 536.6 | |
Note: All figures are rounded
| Program Activity | Forecast Spending 2011–12 |
Planned Spending | ||
|---|---|---|---|---|
| 2012–13 | 2013–14 | 2014–15 | ||
| Internal Services | 114.4 | 95.4 | 95.3 | 95.2 |
Contribution to the Federal Sustainable Development Strategy (FSDS)
The Federal Sustainable Development Strategy (FSDS) outlines the Government of Canada's commitment to improving the transparency of environmental decision-making by articulating its key strategic environmental goals and targets. The Public Health Agency of Canada ensures that consideration of these outcomes is an integral part of its decision-making processes. In particular, through the federal Strategic Environmental Assessment (SEA) process, any new policy, plan, or program initiative includes an analysis of its impact on attaining the FSDS goals and targets. The results of SEAs are made public when an initiative is announced, demonstrating the department's commitment to achieving the FSDS goals and targets.
The Public Health Agency of Canada contributes to Theme IV – Shrinking the Environmental Footprint as denoted by the visual identifier(s) below:
 Theme 4: Shrinking the Environmental Footprint - Starting with the Government
Theme 4: Shrinking the Environmental Footprint - Starting with the Government
These contributions fall under the following Program Activities and are further explained in Section II:
For additional details on the Public Health Agency of Canada's activities to support sustainable development, please see Section II of this RPP and Planning for A Sustainable Future: The Public Health Agency of Canada's Departmental Sustainable Development Strategy 2011-2014. For complete details, please see the Federal Sustainable Development Strategy.
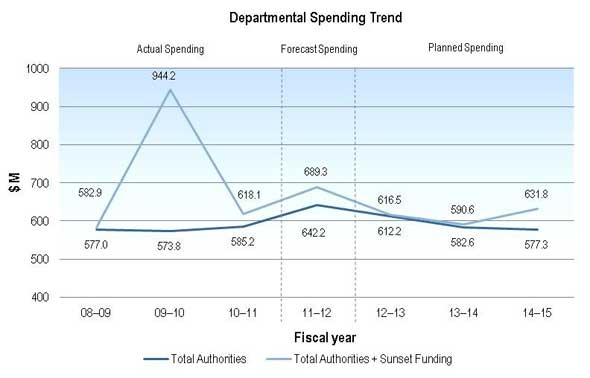
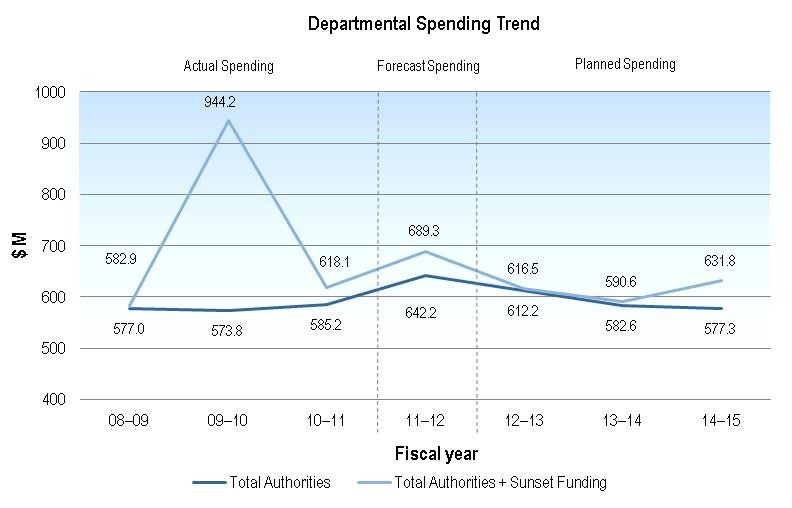
Expenditure Profile
Canada experienced an H1N1 pandemic in 2009–10 which accounts for approximately $310M of additional spending in that year. The Agency also spent $49.7M in the same year on the Hepatitis C Health Care Services Program which provides funding to the provinces to compensate for the care of individuals infected with hepatitis C. This program provides payments every five years until 2014–15. These two items caused a significant change in spending in comparison to other years.
Starting in 2012–13, planned spending will decrease by $72.7M. This can be largely explained by reduced funding of $33.9M for various time-limited projects that are near completion, such as $20.7M for the installation of a new influenza fill line. In addition, one-time funding for 2011–12—consisting of $15.3M to cover severance payouts due to revisions in collective agreements and $18.1M of funds carried forward from 2010–11—will not be available in 2012–13. Finally, $5.9M will be transferred out for the creation of Shared Services Canada.
In 2013–14, PHAC spending decreases by $25.9M mainly as a result of the completion of the initiative to address sport and recreation injuries among Canadian children and youth as well as planned reductions in funding for the JC Wilt Laboratory expansion and the replenishment of the National Antiviral Stockpile.
In 2014–15, Agency spending increases by $41.2M as the final payment of the Hepatitis C Health Care Services Program is made. This increase is partially offset by the planned sunset of initiatives such as Genomics Research and Development and the Lung and Neurological Diseases Initiative as well as the completed replenishment of the National Antiviral Stockpile.
{kind=link}
[enlarge]
{kind=link}
Estimates by Vote
For information on our organizational appropriations, please see the 2012–13 Main Estimates.