
Common menu bar links
Breadcrumb Trail
ARCHIVED - Canadian Institutes of Health Research
 This page has been archived.
This page has been archived.
Archived Content
Information identified as archived on the Web is for reference, research or recordkeeping purposes. It has not been altered or updated after the date of archiving. Web pages that are archived on the Web are not subject to the Government of Canada Web Standards. As per the Communications Policy of the Government of Canada, you can request alternate formats on the "Contact Us" page.
 Minister's Message
Minister's Message
I am very pleased to present the 2008-2009 Departmental Performance Report (DPR) for the Canadian Institutes of Health Research (CIHR).
The Government of Canada is pursuing a multi-year strategy to promote a better quality of life in Canada through science and technology while creating jobs and economic growth.
CIHR has been a valuable partner in this Government's science and technology strategy. Through health research and partnerships across the country, the organization has promoted the health and well being of Canadians by improving the effectiveness and efficiency of the health care system.
Over the last year the CIHR has established a research consortium to advance cancer stem cell research and funded important research into obesity, diabetes, cardiovascular disease, mental health and improving the health of children suffering from asthma and allergies. It has also participated in international research with the United States on cancer and with France on Alzheimer's disease.
The funding of 134 new Canada Research Chairs over the past year at universities across the country has enhanced Canada's international science reputation and its ability to attract the brightest minds from around the globe. The significant support provided for the chairs and their research programs is expected to support well over 500 Canadian and international doctoral students each year.
Through its partnerships with industry, the CIHR has continued to facilitate the commercial application of researchers' findings. Through its innovative knowledge translation programs, CIHR is bringing researchers, clinicians and policy makers together to translate research results into improved treatments and health services.
Through its continued work as leader of the Pandemic Preparedness Strategic Research Initiative (PPSRI), the CIHR has continued to support influenza and pandemic preparedness research in Canada. This initiative, which includes research projects ranging from vaccine development to virus tracking, has helped Canada prepare for the emergence of new infectious diseases, including H1N1 influenza.
This past year, CIHR also partnered with Health Canada to develop the Drug Safety and Effectiveness Network (DSEN), a national research network that will help assess the risks and benefits of medications currently on the market.
These and other initiatives demonstrate both CIHR's commitment to and effectiveness in promoting excellence in health research; research that will continue to improve the lives of Canadians for generations to come.
Leona Aglukkaq
Minister of Health
Government of Canada
Section I: Departmental Overview
Raison d'être & Responsibilities
CIHR is the Government of Canada's premier health research funding agency. It was created in June 2000 by the CIHR Act with a mandate "to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system".
CIHR responds to the evolving needs of health research by:
- supporting outstanding research, both investigator-driven and strategic (i.e. targeted on priority areas), across the full spectrum of health research;
- building research capacity by supporting researchers in under-developed areas and training the next generation of health researchers; and
- promoting knowledge translation, so that the results of research are transformed into relevant applications (policies, practices, procedures, products and services), that have health and economic benefits.
CIHR has created 13 institutes. These institutes are not "bricks-and-mortar" buildings but communities of experts. In its topic area, each of CIHR's 13 Institutes supports a broad spectrum of research: biomedical, clinical, health services and systems, and population and public health. Institutes form national research networks linking researchers, funders and knowledge users across Canada to work on priority areas. This innovative structure has been hailed as a global best practice and supports a problem-based, multidisciplinary and collaborative approach to health research.
CIHR is governed by a Governing Council of 20 members. The President of CIHR serves as its Chair, while the Deputy Minister of Health is an ex-officio and non-voting member. CIHR reports to Parliament through the Minister of Health and, as such, plays a key role in the Health Portfolio.
CIHR works closely with Natural Sciences and Engineering Research Council (NSERC) and Social Sciences and Humanities Research Council (SSHRC), the two Granting Councils of the Industry portfolio, to share information and co-ordinate efforts. The three Councils collectively manage several flagship programs for the Government of Canada, including the Networks of Centres of Excellence Program, the Canada Graduate Scholarships Program and the Canada Research Chairs Program.
In 2008-09, CIHR continued to support the Government of Canada's Science & Technology Strategy. CIHR's focus on excellence and innovation helps ensure that its investments are aligned to the Strategy's key theme of mobilizing S&T to Canada's advantage.
President: Dr. Alain Beaudet, MD, PhD
Annual Spending: $969.4 Million
Head Office: Ottawa
Employees: 403
Institutes: 13
Aboriginal Peoples' Health: Dr. Malcolm King
Aging: Dr. Anne Martin-Matthews
Cancer Research: Dr. Morag Park
Circulatory and Respiratory Health: Dr. Peter Liu
Gender and Health: Dr. Joy Johnson
Genetics: Dr. Roderick McInnes
Health Services and Policy Research: Dr. Colleen M. Flood
Human Development, Child and Youth Health: Dr. Michael Kramer
Infection and Immunity: Dr. Bhagirath Singh
Musculoskeletal Health and Arthritis: Dr. Jane Aubin
Neurosciences, Mental Health and Addiction: Dr. Anthony Phillips
Nutrition, Metabolism and Diabetes: Dr. Philip M. Sherman
Population and Public Health: Dr. Nancy Edwards
CIHR supports the work of over 13,000 health researchers and trainees
Program Activity Architecture (PAA) and Strategic Outcomes
The chart below illustrates CIHR's new Program Activity Architecture (PAA) which came into effect in 2008-09. It has three Strategic Outcomes divided into eight major Program Activities and 19 Sub-Program Activities.
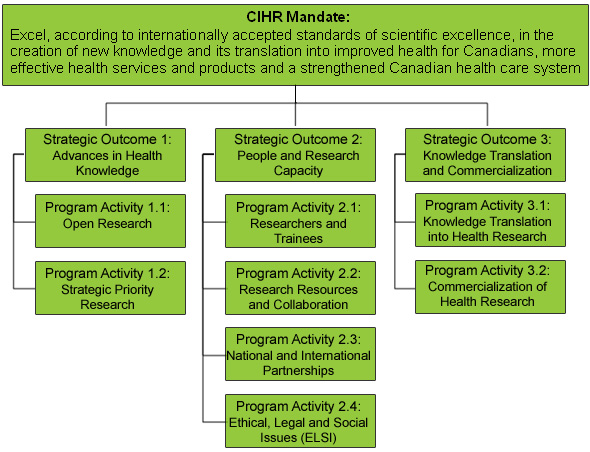
To accomplish its mandate, CIHR provides a range of programs and activities that are designed to support outstanding research, to build health research capacity, and to promote knowledge translation. The following three strategic outcomes will help position Canada as a world leader in the creation and use of health knowledge for the betterment of Canadians and people across the globe. CIHR's strategic outcomes are as follows:
- Advances in Health Knowledge: Canadian health research advances health knowledge and is responsive to current opportunities and priorities.
- People and Research Capacity: A strong and talented health research community with the capacity to undertake health research.
- Knowledge Translation and Commercialization: Health research is translated and adopted into practice, programs and policies that contribute to more effective health services and products, a strengthened health care system, and the improved health of Canadians.
Performance Summary
| Strategic Outcomes | Planned Spending | Total Authorities | Actual Spending |
|---|---|---|---|
| 1.0 Advances in Health Knowledge | $ 585.2 | $ 618.1 | $ 625.5 |
| 2.0 People and Research Capacity | $ 275.1 | $ 278.6 | $ 273.9 |
| 3.0 Knowledge Translation and Commercialization | $ 68.3 | $ 77.3 | $ 70.0 |
| TOTAL | $ 928.6 | $ 974.0 | $ 969.4 |
Total Authorities:
During 2008-09, CIHR's total authorities increased by $45.4M due primarily to a $34M base budget increase announced in the 2008 Federal Budget. In addition, funding for the launch of several new key programs was provided: $4.4M for the Centres of Excellence for Commercialization and Research (CECR) Program (offset by a reduction of $1.4M for the Networks of Centres of Excellence Program), $1.7M for grants through the new Business-Led Networks of Centres of Excellence (BL-NCE) Program, $0.3M to launch the Vanier-Canada Graduate Scholarship (Vanier-CGS) Program and $0.3M for the Canada Foreign Study Supplement Program. CIHR also received net transfers from other federal government departments during the 2008-09 fiscal year totaling $1.8M to fund additional health research projects in key areas including Hepatitis C, the prevention of suicide for aboriginal people, and pandemic preparedness research. Various other administrative type authority increases totaled $4.3M for items such as collective agreement increases and operating budget carry forward.
Actual Spending:
In 2008-09, CIHR's total expenditures were $969.4M which was $4.6M less than total authorities. CIHR lapsed only $0.8M of its Grants Vote during the 2008-09 fiscal year due to careful resource planning and management. A lapse of $3.8M occurred in CIHR's Operating Expenditures Vote due to some authorities being granted to CIHR late in the fiscal year, as well as improvements in operational efficiencies and fewer FTEs being hired than originally planned.
| Planned | Actual | Difference |
|---|---|---|
| 458 | 403 | 55 |
As noted above, CIHR lapsed $3.8M in its Vote 20 (Operating Expenses), due in part to fewer FTE's being hired than originally planned. During 2008-09, CIHR reviewed all of its approved positions to ensure its operations were as efficient as possible. As a result, CIHR reduced its planned FTE's to 410 in its 2009-10 Report on Plans and Priorities.
CIHR also relies on the services of over 2,200 researchers who provide their time each year, without renumeration, to serve on peer review panels that review over 6,000 applications annually.
| Performance Indicators | Targets | 2008-09 Performance |
|---|---|---|
| Canadian ranking in health research expenditures compared to international levels. | Maintain or increase international ranking in health research expenditures. | According to the most recent data, Canada, at 8.6%, ranked among the top five out of the 29 OECD countries studied in terms of health related research and development in government budgets as a percentage of the Gross Domestic Product (GDP). |
| Changes in health practices, programs or policies and improvements in service delivery or health informed by CIHR-funded research. | Evidence of changes in health practices, programs, policies, health service delivery, or health due to the work of CIHR funded researchers. | Changes in health practices, reports from the Institutes and other sources show that CIHR-funded research has had a positive impact on health practices, programs, policies and health service delivery. This is consistent with the findings of a 2006 study by the Council of Canadian Academies which found that Canada is strong in the health and life sciences, relative to other countries, in a number of areas that coincide with CIHR’s priorities. For example: In 2008-09, CIHR brought together private, non-governmental, voluntary and government organizations to further research and apply findings to improve the quality of life of older individuals living with cognitive impairment. CIHR’s work has led other organizations to increase their research in this area. The Canadian Lifelong Health Initiative (CLHI) is a groundbreaking set of large cohort studies targeting birth, chronic disease and aging. It will track the health of thousands of Canadians over many years and generate new knowledge of how environmental, social, life-style, genetic and behavioural factors affect health across the lifespan. Quality of care toward and at the end of life will soon become one of the most important health care issues facing this country. The need for informed decision making by clinical practitioners and policy makers will become critical. CIHR-funded research on overcoming barriers to communication through the use of a Palliative Performance Scale (PPS) has contributed to the growing evidence base needed to support the policy and practice of palliative care in Canada. |
| Number of publications resulting from CIHR-funded research. | Maintain or increase international ranking in health research publications. | Canada ranked 10th in relation to international medical research publications per billion dollars of Gross Domestic Product (GDP). The Canadian share has been steadily rising since 2000, to reach 5% of the world’s total in 2007, the most recent year for which data is available. Canada also ranks in the top ten of OECD countries in terms of the distribution of scientific articles by the field of health research as a percentage of total scientific articles. Canada’s average relative citation (ARC) factor in medical research for 2007 was 1.34, well above the global average of 1.0. As a result Canada ranks 7th world-wide, a significant improvement from its rank of 13th in 2002. |
| Program Activity | 2007-08 Actual Spending |
2008-09 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| 1.1 Open Research | $ 426.4 | $ 462.6 | $ 462.6 | $ 470.9 | $ 493.9 | An Innovative and Knowledge-Based Economy |
| 1.2 Strategic Priority Research | $ 113.1 | $ 122.6 | $ 122.6 | $ 147.2 | $ 131.6 | |
| Total | $ 539.5 | $ 585.2 | $ 585.2 | $ 618.1 | $ 625.5 | |
Change in Spending:
Actual spending increased by $86.0M over the prior fiscal year. CIHR's spending on its largest program, the Open Operating Grants Program (OOGP), increased by $28.7M due to increased application pressure and the increased costs of conducting research. Expenditures also increased in several other priority areas including $10.6M for clinical research, $3.7M for pandemic preparedness, $2.5M for regenerative medicine, $1.9M for HIV/AIDS research, $0.9M for global health and $0.8M for Fabry's Disease. In addition, CIHR's 13 Institutes invested an additional $18.7M in strategic priority operating grants.
Total Authorities:
CIHR's total authorities increased by $32.9M during 2008-09. Of this increase, $30.9M related to the base budget increase from the 2008 Federal Budget. CIHR also received an additional $2.0M in authorities via transfers from other government departments to fund additional grants in key strategic priority areas of health research (including Hepatitis C research and pandemic preparedness research).
Actual Spending:
Actual spending associated with this Strategic Outcome was $7.4M higher than total authorities as a result of the reallocation of funds from the other two Strategic Outcomes. More specifically, measures were undertaken to ensure that the target of a minimum of 800 high quality grants under the Open Operating Grant Program would be met. This program is critical as it is the foundation on which a strong and diverse research enterprise is built.
| Performance Indicators | Targets | 2008-09 Performance |
|---|---|---|
| Number and types of PhD graduates in health research or related domains in Canada by year. | Maintain or increase international ranking. | The number of PhD graduates in Canada is increasing slowly, as is the number of graduates per capita which has increased from 42 per 100,000 population (aged 20-39) to 48 per 100,000 in six years. However, Canada’s international ranking in the number of graduated PhD students compared to other OECD countries was next to last in both 1998 and 2006, the only years for which CIHR has data. |
| Average time to completion of degrees compared to general population. | Maintain or accelerate time to degree for CIHR award holders. | According to the preliminary results of the recent evaluation of the Canada Graduate Scholarships (CGS) Program, Master’s students supported through CGS took slightly less time to obtain their degree while Doctoral students supported through CGS took the same time to obtain their degree as students funded from other sources. |
| Number and types of investigators funded. | Maintain number and diversity (by Institute) of investigators funded. | The number and diversity of investigators funded by CIHR has increased in all research sectors, at all the Institutes and for many different types of research. |
| Program Activity | 2007-08 Actual Spending |
2008-09 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| 2.1 Researchers and Trainees | $ 202.3 | $ 196.1 | $ 196.1 | $ 198.2 | $ 188.9 | An Innovative and Knowledge-Based Economy |
| 2.2 Research Resources and Collaboration | $ 68.0 | $ 50.9 | $ 50.9 | $ 52.0 | $ 58.9 | Healthy Canadians |
| 2.3 National and International Partnerships | $ 24.0 | $ 25.2 | $ 25.2 | $ 25.4 | $ 23.7 | |
| 2.4 Ethical, Legal and Social Issues (ELSI) | $ 2.2 | $ 2.9 | $ 2.9 | $ 3.0 | $ 2.4 | |
| Total | $ 296.5 | $ 275.1 | $ 275.1 | $ 278.6 | $ 273.9 | |
Change in Spending:
Actual spending decreased by $22.6M compared to 2007-08 mainly due to reduced spending on the Researchers and Trainees Program Activity. With the expansion to the Canada Graduate Scholarship (CGS) Program and in recognition that many researchers and trainees benefit from their participation in Open Operating Grant Program (OOGP) funded projects, it was determined that some funding from this Strategic Outcome could be transferred to Strategic Outcome #1.
Total Authorities:
Total authorities increased by $3.5M during the year which was mainly due to the base budget increase from Budget 2008. As well, some additional authorities for specific programs were also provided including $0.3M for the Canadian Foreign Supplement Program and $0.3M for the Vanier-CGS Program.
Actual Spending:
Actual spending was $4.7M less than the total authorities approved, reflecting the decision to reallocate funding towards the OOGP.
| Performance Indicators | Targets | 2008-09 Performance |
|---|---|---|
| Changes in health practice, programs or policies informed by CIHR-funded research, improvements in service delivery informed by CIHR-funded research. | Evidence of changes in health practices, programs, policies, health service delivery or health due to work of CIHR funded researchers. | The reports of its Institutes and other sources have provided some evidence of the positive impact of CIHR-funded research on health practices, programs, policies and health service delivery. For example: The Canadian Dementia Knowledge Translation Network (CDKTN) was established to accelerate the uptake of evidence for improved diagnosis, treatment and care in dementia by linking researchers to research users (e.g. front-line workers). CDKTN is a network for translation and exchange of research in Alzheimer disease and dementia. CIHR-supported researchers developed innovative genetic techniques, involving a gene called piggyback, that make it possible to develop pluripotent stem cells from anyone, and to direct these stem cells into becoming the type of cells needed for cell replacement of a diseased tissue. This research should bring stem cell treatment for many diseases to the clinic. CIHR is helping to resolve the question, “Is it better and safer to perform bypass surgery while a patient is on a heart-lung machine or directly on a beating heart?” by funding the world’s largest cardiac surgery clinical trial, involving 4,700 patients in 100 cardiac surgical centres across 16 countries. Led by Drs. André Lamy and Salim Yusuf at Hamilton Health Sciences, McMaster University, the 7.5 year CORONARY trial will investigate the differences in outcomes of the two techniques during coronary artery bypass surgery. “This trial will change practice around the world and play a key role in reducing complications for patients who undergo cardiac surgery, “ says Dr. Lamy. |
| Commercial activity – products (IP), companies and employment generated as a result of CIHR-funded projects. | Evidence of commercial activity due to work of CIHR funded researchers. | The reports of the Institutes and other sources have provided some evidence that CIHR-funded research has led to significant commercial activity. For example: A Network Centres of Excellence (NCE) evaluation found that, while many of the positive outcomes of the NCE Program are shared with other network-related programs, it performs better than these programs in some key areas, such as the creation of structured networks, the establishment of intersectoral partnerships, and knowledge utilization — in particular, the commercialization of research findings. A preliminary report on patents awarded to Canadian health scientists from 2002 to 2007 shows that CIHR has supported more than 70% of those inventors and innovators obtaining patents in health during that period. Dr. Charles Bernstein and his team focused on the hypothesis that colon tumours shed both cells and chemicals that are characteristic of the tumour. The team used magnetic resonance spectroscopy and advanced mathematical methods to produce a chemical signature of stool samples prior to a patient undergoing colonoscopy, thus eliminating the need for invasive colonoscopy for patients who tested negative. The team has published their findings, established two patents on the technology, and are collaborating with a North American company to bring the technology to market. |
| Changes in the health and quality of life of Canadians in areas of CIHR investment as a result of CIHR-funded projects. | Maintain or increase international ranking related to quality of life. | Numerous studies using different methodologies seek to measure quality of life. Canada’s ranking is generally high and occasionally is very high. For example: Canada ranks 3rd worldwide in terms of the Human Development Index, which considers measures of life expectancy, literacy, educational attainment and per capita Gross Domestic Product (GDP). Canada ranks 11th, among 24 OECD countries in terms of overall health performance and third overall amongst G7 countries in terms of life expectancy. Canada’s health care system ranks 30th out of 191 nations by the World Health Organization based on measures of the health status of the population, the responsiveness of the health system and national health expenditures. Canada ranks 23rd among 30 countries according to the Euro-Canada Health Consumer Index that incorporates measures of patient rights and information wait times for various treatments, clinical outcomes and provision of pharmaceuticals. |
| Program Activity | 2007-08 Actual Spending |
2008-09 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| 3.1 Knowledge Translation of Health Research | $ 39.8 | $ 40.8 | $ 40.8 | $ 43.6 | $ 41.5 | Healthy Canadians |
| 3.2 Commercialization of Health Research | $ 98.3 | $ 27.5 | $ 27.5 | $ 33.7 | $ 28.5 | An Innovative and Knowledge-Based Economy |
| Total | $ 138.1 | $ 68.3 | $ 68.3 | $ 77.3 | $ 70.0 | |
Change in Spending:
Actual spending was $68.1M less than 2007-08 spending due in large part to $69.1M of one-time funding for the launch of the Centres of Excellence in Commercialization and Research (CECR) Program. That program was announced as part of the 2007 Federal Budget with the initial recipients receiving their funding up-front in the form of a lump sum.
Total Authorities:
Total authorities increased by $9.0M during the year. This increase was due primarily to $4.4M additional funding announced for the second round of the CECR Program grants and $1.7M of funding for the new Business Led- Networks of Centres of Excellence (BL-NCE) Program. Additionally, CIHR invested an additional $3.8M in knowledge translation and commercialization activities as a result of the base budget increase in the 2008 Federal Budget.
Actual Spending:
Actual spending was $7.3M less than total authorities. Program spending on Knowledge Translation grant programs was $2.1M less than originally planned because CIHR received some of its additional authorities very late in the fiscal year, therefore not having time to launch new funding opportunities. Program spending in certain industry-partnered programs, such as the Small and Medium Enterprise research program and the CIHR and Canada's Research Based Pharmaceutical companies, fell short of planned spending by $5.2M. Surplus funding was reallocated to the Open Operating Grants Program (OOGP) in Strategic Outcome #1.
Contribution of Priorities to Strategic Outcomes
This table reports on progress with respect to the strategic priorities identified in CIHR's 2008-2009 Report on Plans and Priorities (RPP) Section IV.
| Operational Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
| Renewing CIHR's strategic priorities | Previously committed to | Successfully Met
|
Strategic Outcomes 1, 2 & 3 |
| Building a better and simpler CIHR | On-going | Somewhat Met
|
Strategic Outcomes 1, 2 & 3 |
| Enhancing effectiveness of peer review | On-going | Successfully Met
|
Strategic Outcomes 1 & 2 |
| Utilizing technology to enhance service delivery | On-going | Successfully Met
|
Strategic Outcomes 1 & 2 |
| Evaluating our performance | On-going | Successfully Met
|
Strategic Outcomes 1, 2 & 3 |
| Improving reporting of health research and impacts | On-going | Successfully Met
|
Strategic Outcomes 1, 2 & 3 |
| Management Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
| Ensuring a committed workforce | On-going | Successfully Met
|
Strategic Outcomes 1, 2 & 3 |
| Advancing modern management practices | On-going | Successfully Met
|
Strategic Outcomes 1, 2 & 3 |
| Ensuring the smooth Scientific Director/Host Institution transitions for five CIHR Institutes | Previously committed to | Successfully Met
|
Strategic Outcomes 1, 2 & 3 |
Risk Analysis
CIHR's programs and priorities are often affected by factors outside its control. Nevertheless, CIHR continuously assesses opportunities, challenges and risks at three levels: strategic, programs and corporate. For environmental scanning and response development at a strategic level, each of the 13 Institutes relies on its Advisory Board to provide a wide variety of perspectives on health and health research issues. These Boards identify threats to the health of Canadians and opportunities for rapid advances in health knowledge and develop strategic research initiatives in response. At the program level, CIHR managers continuously monitor the different types of support required for researchers and the appropriateness of the design of CIHR's research funding mechanisms. At the corporate level, each of CIHR's functional areas (e.g. Human Resources, Finance and Evaluation) regularly reviews the effectiveness and efficiency of CIHR's operations to identify weaknesses and opportunities for improvement. Risks and challenges for CIHR are, by the nature of its business, horizontal and cut across all strategic outcomes rather than being specific to any one strategic outcome.
CIHR has to maintain a balance between supporting long-term research projects, thereby locking-in future funds, and reserving enough future funding for new opportunities that, although currently unknown, are sure to present themselves in future years. To better manage this balancing act, CIHR has introduced investment modelling to better forecast the future impacts of current funding decisions and to introduce the concept of "steady state" dynamics to ensure relative stability in the number of new applications funded annually and success rates across time. CIHR also developed a five year Investment Road Map to help plan the future evolution of its programming and to ensure an appropriate balance between investigator-driven "open" research, and research that is targeted at priorities identified by CIHR and Government.
Evaluating the results and outcomes of CIHR-funded research is challenging as causal links between health research inputs, outputs and impacts are difficult to trace when knowledge develops incrementally over time and through multiple channels. Attribution of credit for research impacts can also be complex, as impacts often result from a number of research projects carried or funded either collaboratively or independently in the same and/or different countries. By using a framework and indicators for measuring the value of investments in health research, CIHR anticipates going beyond the evaluation of outputs associated with individual programs or grants to broader conclusions around the results and outcomes of health research.
In 2008-09 CIHR developed and piloted its end-of-grant reporting tool which will allow researchers to document the impacts of their research. Over time this tool will provide significant information on the results of the research funded by CIHR and will provide a framework to guide future programming choices and resource allocation.
Finally, CIHR continues to be challenged by the increasing number of high-quality applications submitted by researchers. CIHR relies on peer review to assess and rank applications but the increase in CIHR's funding opportunities and applications is putting a strain on the peer review process. In 2008-09, CIHR launched an initiative to ensure the sustainability and continued effectiveness of peer review. The application of technology and the standardization of business processes will make peer review more efficient while measures to rationalize programs and funding opportunities will help contain demand for peers.
Expenditure Profile
CIHR Actual Spending Since 2003-04 (in $ millions)
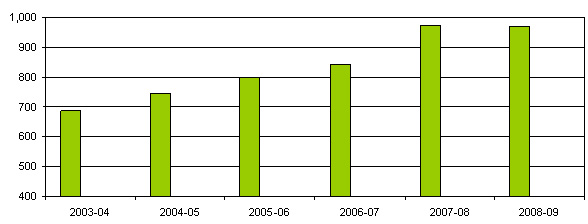
CIHR expenditures increased from $686.2M in 2003-04 to $974.1M in 2007-08, an increase of $287.9M (or 42%) in five years. Since its creation in 2000, CIHR's budget has increased every year until 2008-09 when its spending was marginally less than in the previous year.
| Vote # or Statutory Item (S) | Truncated Vote or Statutory Wording | 2006-07 Actual Spending |
2007-08 Actual Spending |
2008-09 Main Estimates |
2008-09 Actual Spending |
|---|---|---|---|---|---|
| 20 | Operating expenditures | $ 39.4 | $ 42.8 | $ 42.9 | $ 47.2 |
| 25 | Grants | $ 799.7 | $ 926.7 | $ 881.3 | $ 916.9 |
| (S) | Contributions to employee benefit plans | $ 4.2 | $ 4.6 | $ 4.4 | $ 5.3 |
| Total | $ 843.3 | $ 974.1 | $ 928.6 | $ 969.4 | |